TB Granuloma
Lesson 5 of 15 · Detailed pathology
Points of Recognition
- 1Central caseous necrosis
- 2Epithelioid histiocytes with elongated nuclei
- 3Langhans giant cells with peripheral nuclear arrangement
- 4Lymphocytic cuff
- 5Acid‑fast bacilli (AFB) on ZN stain (within giant cells or necrosis)
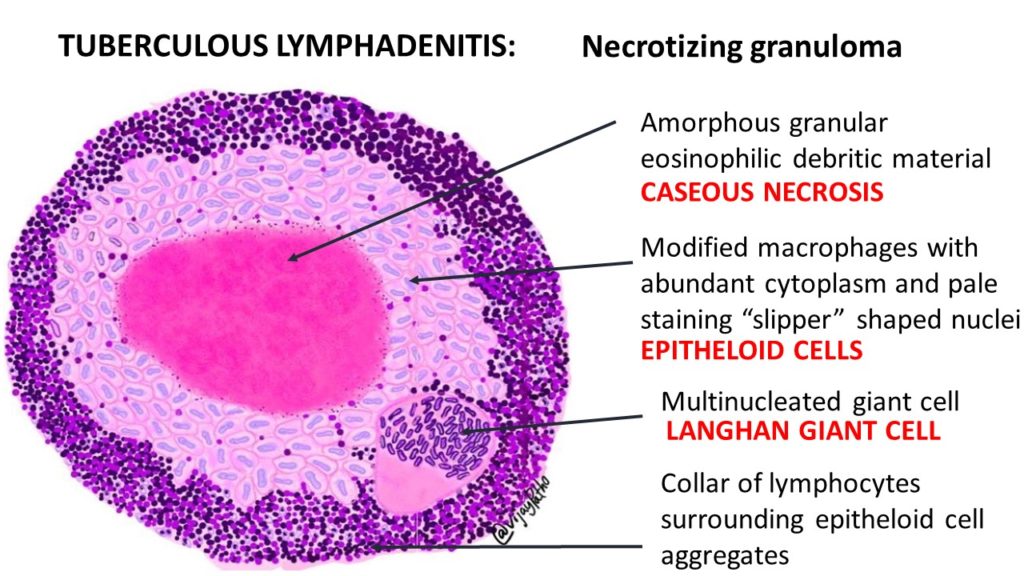
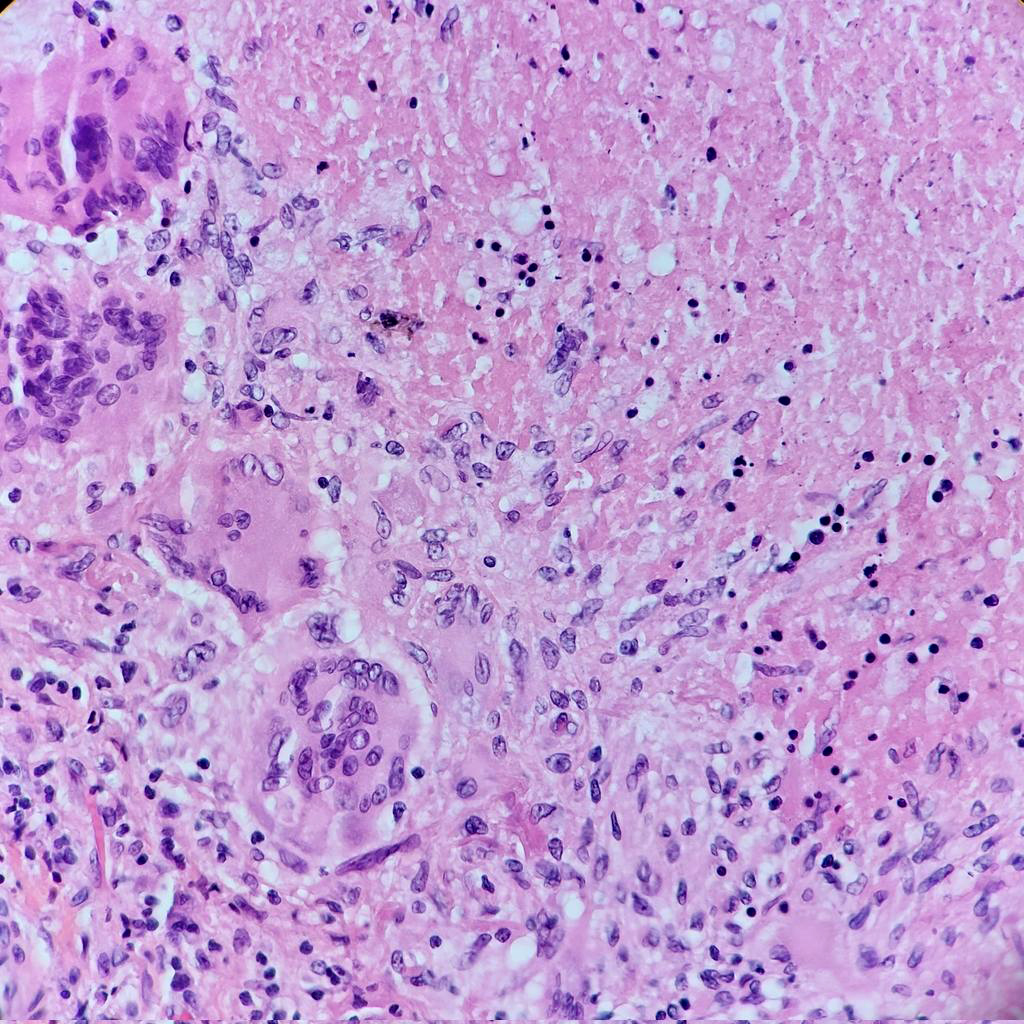
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
A tuberculous granuloma is a classic caseating (necrotic) granuloma caused by Mycobacterium tuberculosis. It consists of central caseous necrosis surrounded by epithelioid macrophages and Langhans giant cells, rimmed by lymphocytes and outer collagen fibrosis — representing a type IV delayed hypersensitivity reaction.
General / Essential Features
- Central caseous (cheese-like) necrosis — amorphous eosinophilic acellular material
- Langhans giant cells: peripheral horseshoe arrangement of nuclei
- Surrounding epithelioid macrophages (transformed from monocytes)
- Rim of lymphocytic infiltration around the granuloma
- Collagen strands (fibrosis) forming the outer boundary
- ZN (Ziehl–Neelsen) stain demonstrates acid-fast bacilli (AFB)
Sites
- Lung (primary complex: subpleural focus + hilar lymph node)
- Lymph nodes (cervical, mediastinal, mesenteric)
- Pleura, peritoneum (miliary/disseminated TB)
- Gut (ileocaecal junction — most common GI site)
- Bone and joints (Pott's spine: vertebral TB)
- Kidneys, adrenal glands, CNS (tuberculomas)
Pathophysiology
M. tuberculosis is phagocytosed by alveolar macrophages but resists killing via inhibition of phagosome–lysosome fusion. Antigen presentation activates CD4+ Th1 cells, which release IFN-γ, activating macrophages to form epithelioid cells and fuse into giant cells. Cytokine-mediated hypoxia and direct bacterial toxins cause central caseation. Containment failure leads to cavitation and dissemination.
Etiology
- Mycobacterium tuberculosis: aerobic, acid-fast bacillus
- Mycobacterium bovis: zoonotic, from unpasteurised dairy
- Risk factors: HIV/AIDS, malnutrition, diabetes, crowded living
- Immunosuppressive therapy (corticosteroids, TNF-α inhibitors)
Clinical Features
- Primary TB: usually asymptomatic; Ghon complex on CXR
- Post-primary TB: productive cough, haemoptysis, fever, night sweats, weight loss
- Pleural effusion: exudative, lymphocyte-predominant
- Extrapulmonary: lymphadenopathy, cold abscess, spinal pain (Pott's)
- Miliary TB: bilateral fine nodular shadows on CXR ('millet seeds')
Diagnosis
- Sputum AFB smear and culture (Lowenstein–Jensen medium — 6–8 weeks)
- GeneXpert MTB/RIF: rapid PCR with rifampicin resistance detection
- Histopathology: caseating granuloma + ZN stain
- Tuberculin skin test (TST/Mantoux) and IGRA (QuantiFERON)
- CXR: upper lobe cavitation, hilar lymphadenopathy
Treatment
- HRZE: Isoniazid + Rifampicin + Pyrazinamide + Ethambutol for 2 months
- Then HR: Isoniazid + Rifampicin for 4 months (total 6 months)
- MDR-TB: longer regimens with second-line drugs (fluoroquinolones, linezolid)
- Corticosteroids: adjunctive in TB meningitis and pericarditis
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test