Chronic Venous Congestion (Liver)
Lesson 12 of 15 · Detailed pathology
Points of Recognition
- 1Dilated central veins and sinusoids
- 2Centrilobular haemorrhagic necrosis (zone 3)
- 3Periportal fatty change (zone 1)
- 4Preserved portal triads
- 5Centrilobular fibrosis in chronic cases
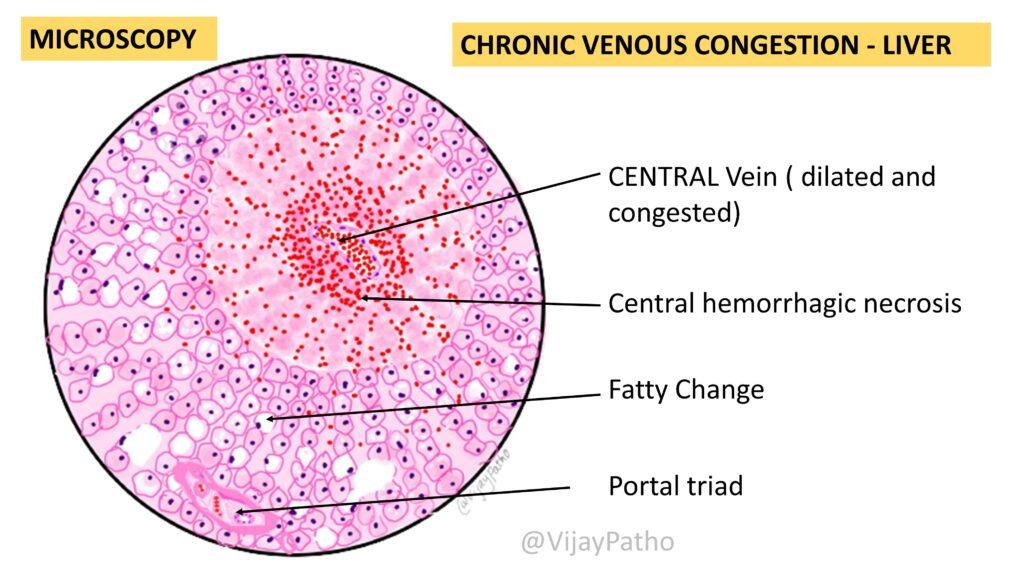
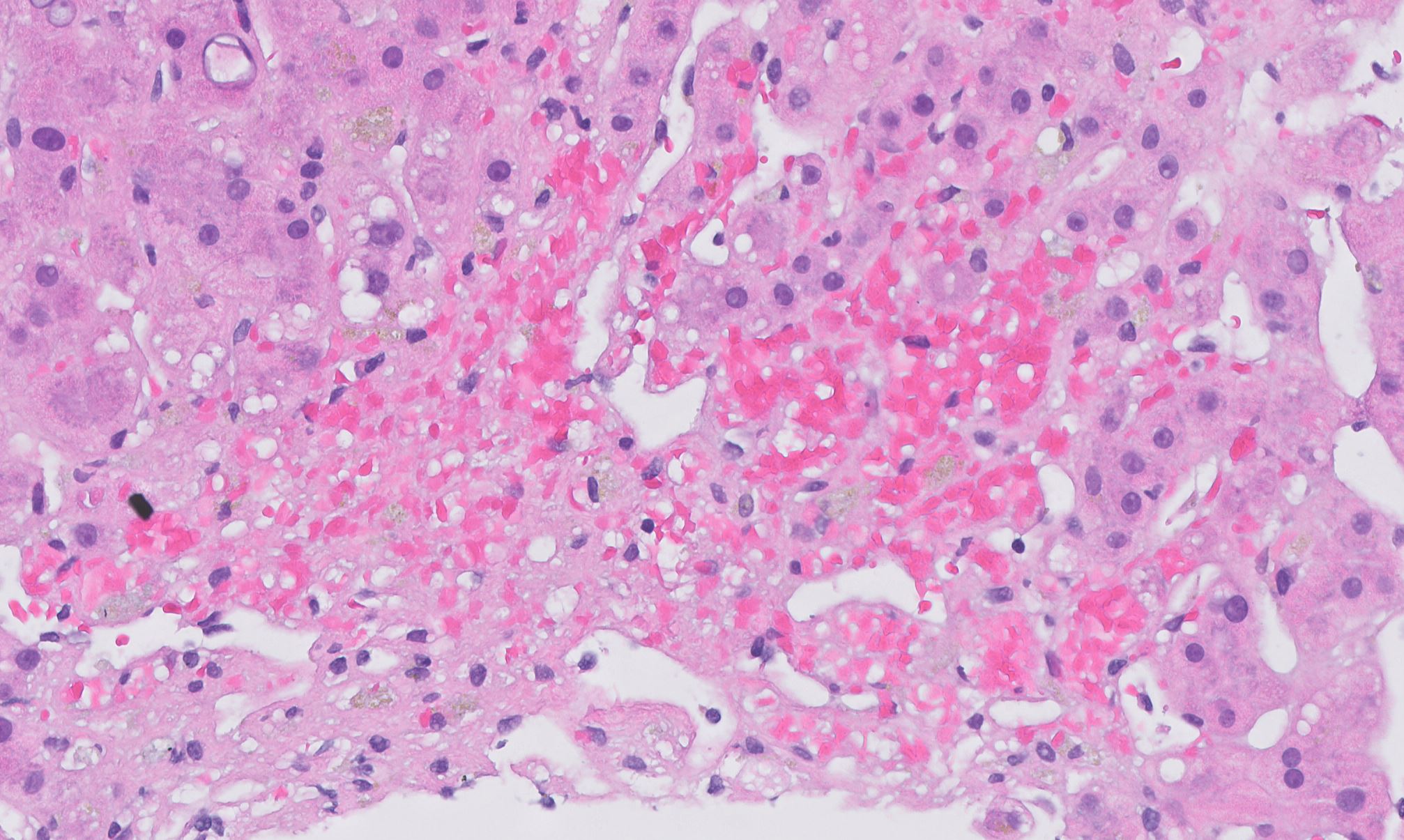
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Chronic venous congestion of the liver (cardiac liver) results from right-sided heart failure causing chronic back-pressure in the hepatic veins. Grossly it produces the 'nutmeg' pattern; histologically there is dilated central veins and sinusoids, centrilobular haemorrhagic necrosis, periportal fatty change, and preserved portal triads.
General / Essential Features
- Dilated central veins and sinusoids (centrilobular)
- Centrilobular haemorrhagic necrosis (zone 3 hepatocytes)
- Eosinophilic hepatocyte cytoplasm in zone 3
- Fatty changes in periportal (zone 1) hepatocytes
- Portal triads relatively preserved
- Chronic cases: centrilobular fibrosis → cardiac cirrhosis
Sites
- Centrilobular (zone 3): primary injury site from venous back‑pressure
- Whole liver affected grossly — 'nutmeg liver' on cut surface
- Hepatic veins and IVC downstream pathology
Pathophysiology
Right heart failure → elevated right atrial pressure → retrograde transmission to hepatic veins → sinusoidal congestion → ischaemic necrosis of centrilobular hepatocytes (zone 3, farthest from portal blood supply). Atrophied hepatocytes with haemorrhagic necrosis appear red; preserved periportal hepatocytes with fatty change appear yellow — producing the nutmeg pattern.
Etiology
- Right heart failure (commonest): IHD, cor pulmonale, cardiomyopathy
- Constrictive pericarditis: Kussmaul's sign, elevated JVP
- Tricuspid regurgitation or stenosis
- Budd–Chiari syndrome: hepatic vein thrombosis — acute variant
Clinical Features
- Signs of right heart failure: raised JVP, peripheral oedema, hepatomegaly
- Pulsatile liver in tricuspid regurgitation
- Mild jaundice and elevated bilirubin
- Ascites in severe cases
- Hepatojugular reflux positive
Diagnosis
- Echocardiography: identifies underlying cardiac pathology
- LFTs: mild elevation of AST/ALT/bilirubin; low albumin in chronic disease
- CT abdomen: patchy 'mosaic' hepatic enhancement
- Liver biopsy: centrilobular congestion, necrosis, fibrosis
Treatment
- Treat underlying cardiac cause: diuretics, ACE inhibitors, beta‑blockers
- Anticoagulation: for Budd–Chiari or thrombotic causes
- Cardiac resynchronisation therapy (CRT) or cardiac transplant in refractory HF
- TIPS: for refractory ascites in cardiac cirrhosis
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test