PathologyAcute Appendicitis
🫀
Pathology Lesson · GI Pathology
Acute Appendicitis
Lesson 1 of 15 · Detailed pathology
PathologyGI Pathology
Points of Recognition
- 1Transmural neutrophilic inflammation
- 2Mucosal ulceration and cryptitis
- 3Luminal obstruction (faecolith or lymphoid hyperplasia)
- 4Hyperaemic serosa with fibrin exudate
- 5Perforation in advanced cases
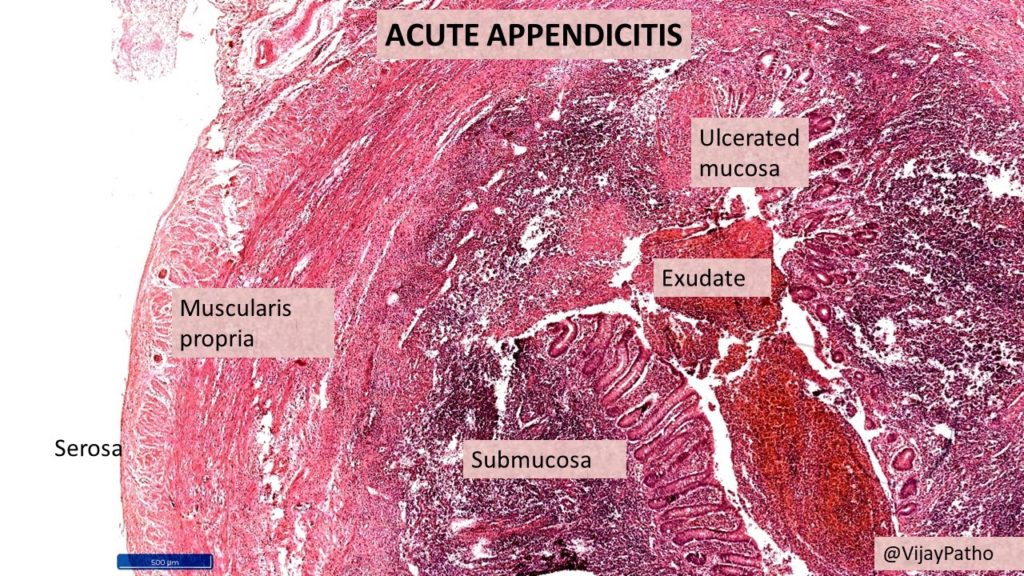
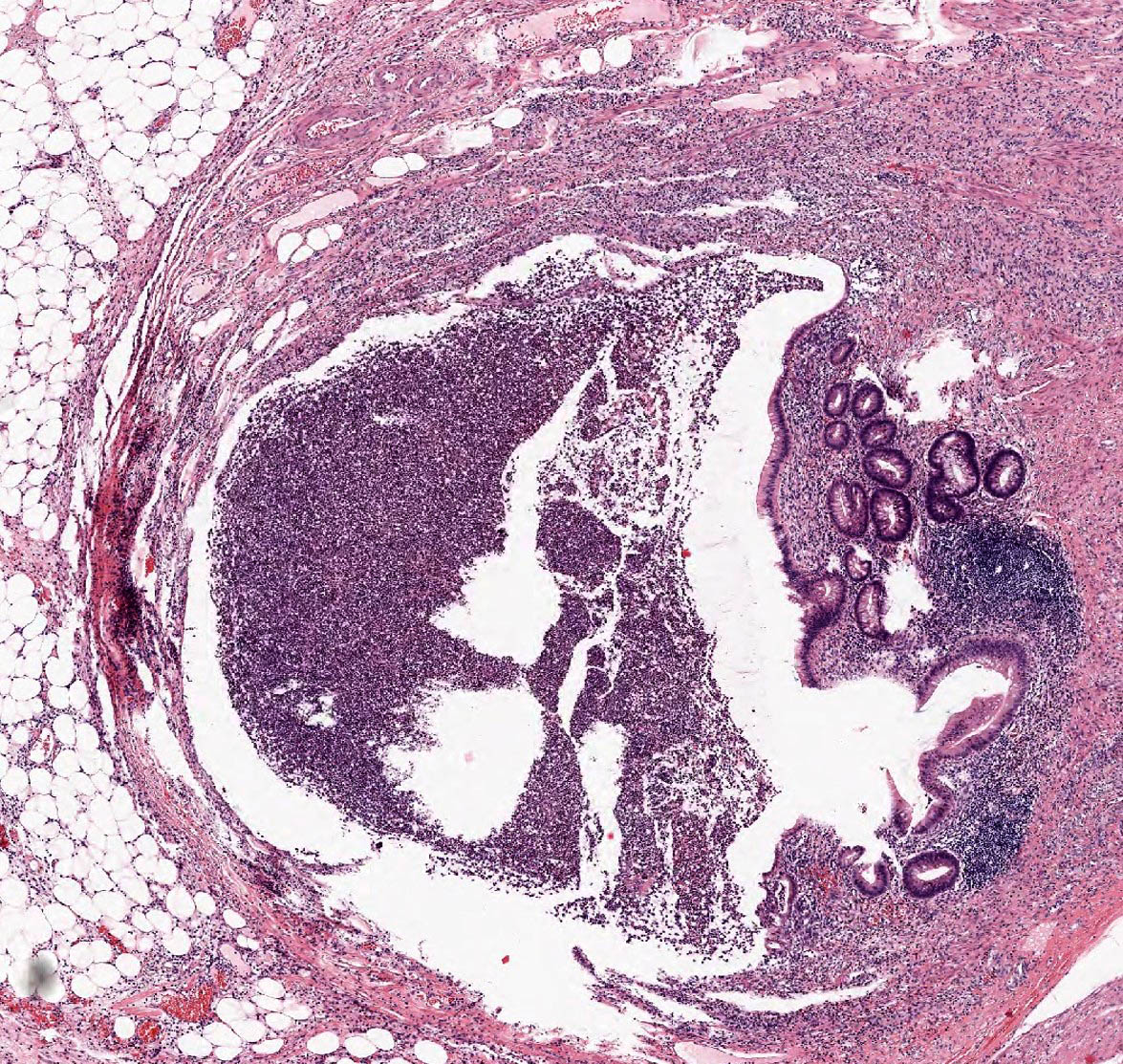
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Acute appendicitis is acute inflammation of the vermiform appendix, most commonly caused by luminal obstruction (faecolith or lymphoid hyperplasia) leading to bacterial overgrowth, mucosal ulceration, and transmural inflammation. It is the commonest surgical emergency of the abdomen.
General / Essential Features
- Hyperplastic lymphoid follicles causing luminal obstruction
- Transmural neutrophilic infiltration of the appendiceal wall
- Neutrophil exudate spreading into the submucosa
- Inflamed and hyperaemic serosal layer
- Fibrin deposition on the peritoneal surface
- Mucosal ulceration overlying the obstructed segment
Sites
- Vermiform appendix (sole site) — tip, body, or base
- Base obstruction increases risk of perforation
- May extend into pericaecal tissues causing pericaecal abscess
- Perforated appendicitis → generalised peritonitis
Pathophysiology
Luminal obstruction raises intraluminal pressure, impairing mucosal blood supply. Enteric bacteria (E. coli, Bacteroides) proliferate, invade the wall, and trigger acute inflammation. Vascular thrombosis causes gangrene; perforation releases contents into the peritoneum.
Etiology
- Faecolith (calcified faecal mass) — most common in adults
- Lymphoid hyperplasia — most common in children (post-viral)
- Parasites (pinworms, Ascaris) — rare
- Tumour obstructing the base (carcinoid, adenocarcinoma)
Clinical Features
- Periumbilical pain migrating to right iliac fossa (McBurney's point)
- Anorexia, nausea, vomiting
- Low-grade fever, rebound tenderness, guarding
- Rovsing sign positive; Psoas sign positive in retrocaecal appendix
- Elevated WBC (neutrophilia), elevated CRP
Diagnosis
- Clinical diagnosis supported by Alvarado score
- Ultrasound: non-compressible, blind-ending tubular structure >6 mm
- CT abdomen: gold standard — periappendiceal fat stranding, appendicolith
- Histopathology post-appendicectomy: confirms diagnosis
Treatment
- Emergency appendicectomy (laparoscopic preferred)
- IV antibiotics (co-amoxiclav, metronidazole) pre- and post-op
- Interval appendicectomy after 6 weeks if appendiceal mass settles conservatively
- Perforation: peritoneal washout, drain placement
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test