PathologyLeiomyoma
🌀
Pathology Lesson · Smooth Muscle Tumour
Leiomyoma
Lesson 6 of 15 · Detailed pathology
PathologySmooth Muscle Tumour
Points of Recognition
- 1Intersecting fascicles of spindle cells
- 2Cigar‑shaped (blunt‑ended) nuclei
- 3Abundant eosinophilic cytoplasm
- 4No nuclear atypia or pleomorphism
- 5Low mitotic count (<5/10 HPF)
- 6Hyaline degeneration (common)
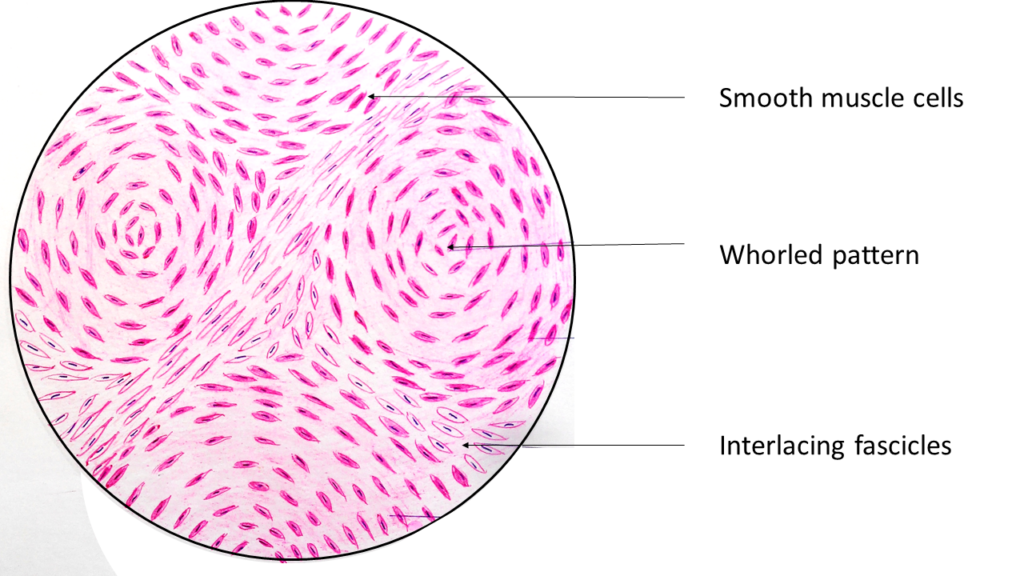
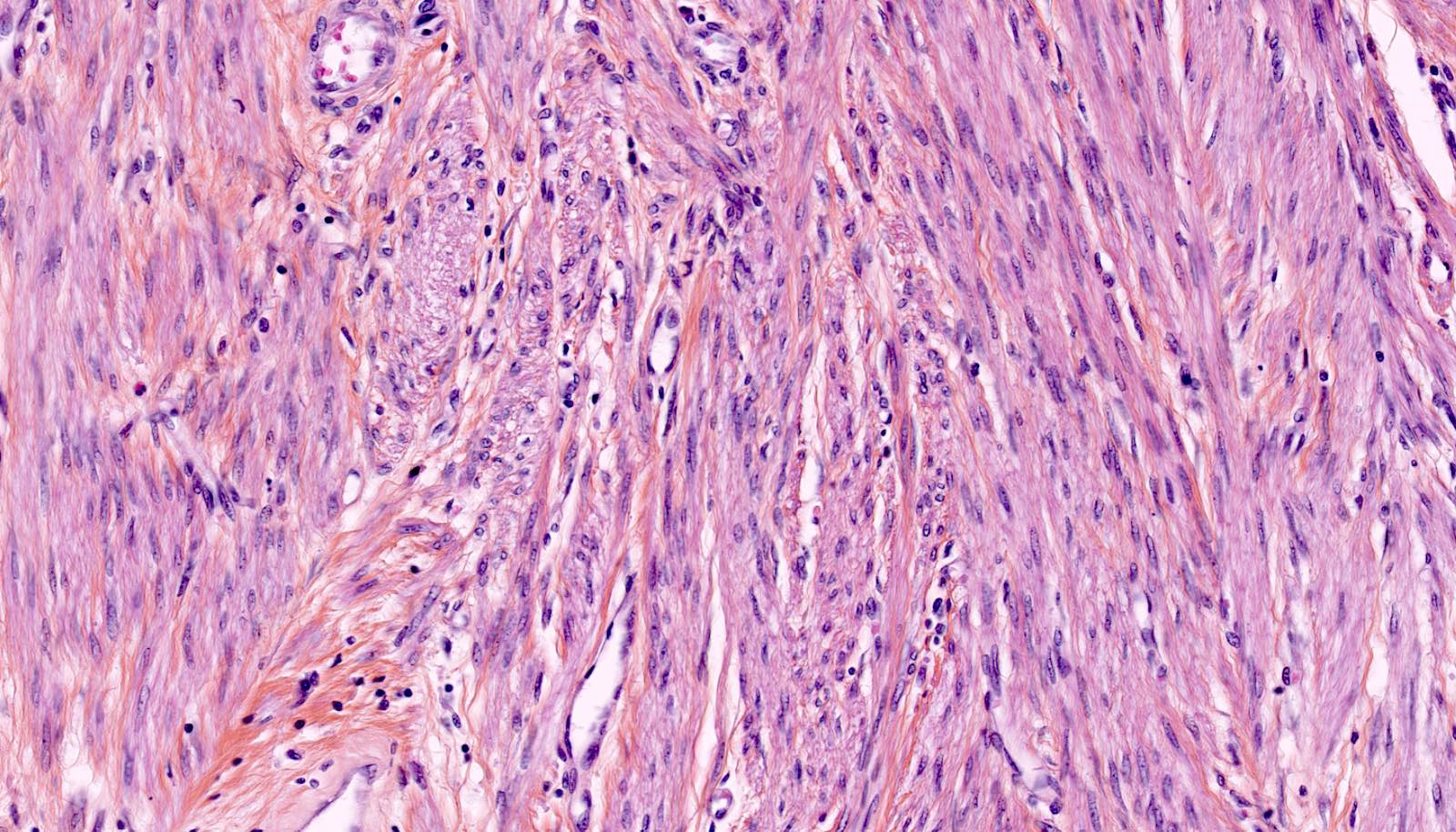
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Leiomyoma (fibroid) is the most common benign tumour of the uterus, arising from smooth muscle of the myometrium. Histologically it consists of intersecting fascicles of bland spindle-shaped smooth muscle cells with cigar-shaped nuclei, eosinophilic cytoplasm, and low mitotic activity.
General / Essential Features
- Intersecting fascicles of spindle-shaped smooth muscle cells
- Elongated cigar-shaped (blunt-ended) nuclei — no significant atypia
- Abundant eosinophilic cytoplasm
- Variable collagen between muscle bundles
- No significant nuclear pleomorphism or hyperchromasia
- Low mitotic activity (<5 mitoses per 10 HPF)
Sites
- Intramural: within myometrial wall — most common (70%)
- Subserosal: projecting from outer uterine surface — can become pedunculated
- Submucosal: bulging into endometrial cavity — causes heavy bleeding
- Cervical fibroids: rare
- Broad ligament fibroids: may compress ureter
Pathophysiology
Oestrogen and progesterone drive growth; leiomyomas have increased oestrogen receptor expression. Somatic mutations in MED12 (>70% of cases) drive clonal expansion. Growth is slow; menopause causes regression. Secondary degenerative changes: hyaline (commonest), cystic, red (carneous — in pregnancy), calcific.
Etiology
- Hormonal: oestrogen-dependent — increases in reproductive years, regresses post-menopause
- MED12 mutation: most common somatic driver
- Genetic predisposition: Black women have 3–5× higher incidence
- Obesity, nulliparity, early menarche — risk factors
Clinical Features
- Heavy menstrual bleeding (HMB) — leading to iron-deficiency anaemia
- Dysmenorrhoea and pelvic pain
- Urinary frequency or retention (pressure on bladder)
- Subfertility: submucosal fibroids distort endometrial cavity
- Abdominal mass in large fibroids
- Many are asymptomatic — incidental finding on ultrasound
Diagnosis
- Pelvic ultrasound: hypoechoic, well-defined myometrial masses
- MRI pelvis: gold standard for mapping fibroid location pre-surgery
- Hysteroscopy: for submucosal fibroids
- Histopathology: spindle cells, cigar nuclei, low mitoses
Treatment
- Conservative: GnRH analogues (leuprolide) to shrink fibroids pre-surgery
- Mifepristone or ulipristal acetate: SPRM for medical management
- Myomectomy: surgical removal preserving fertility
- Hysterectomy: definitive — for completed family or severe symptoms
- Uterine artery embolisation (UAE): minimally invasive alternative
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test