Fatty Liver
Lesson 11 of 15 · Detailed pathology
Points of Recognition
- 1Macrovesicular steatosis (large vacuole, peripheral nucleus)
- 2Microvesicular steatosis (multiple small vacuoles, central nucleus)
- 3Ballooning degeneration of hepatocytes
- 4Mallory‑Denk bodies (eosinophilic inclusions)
- 5Lobular inflammation (mixed)
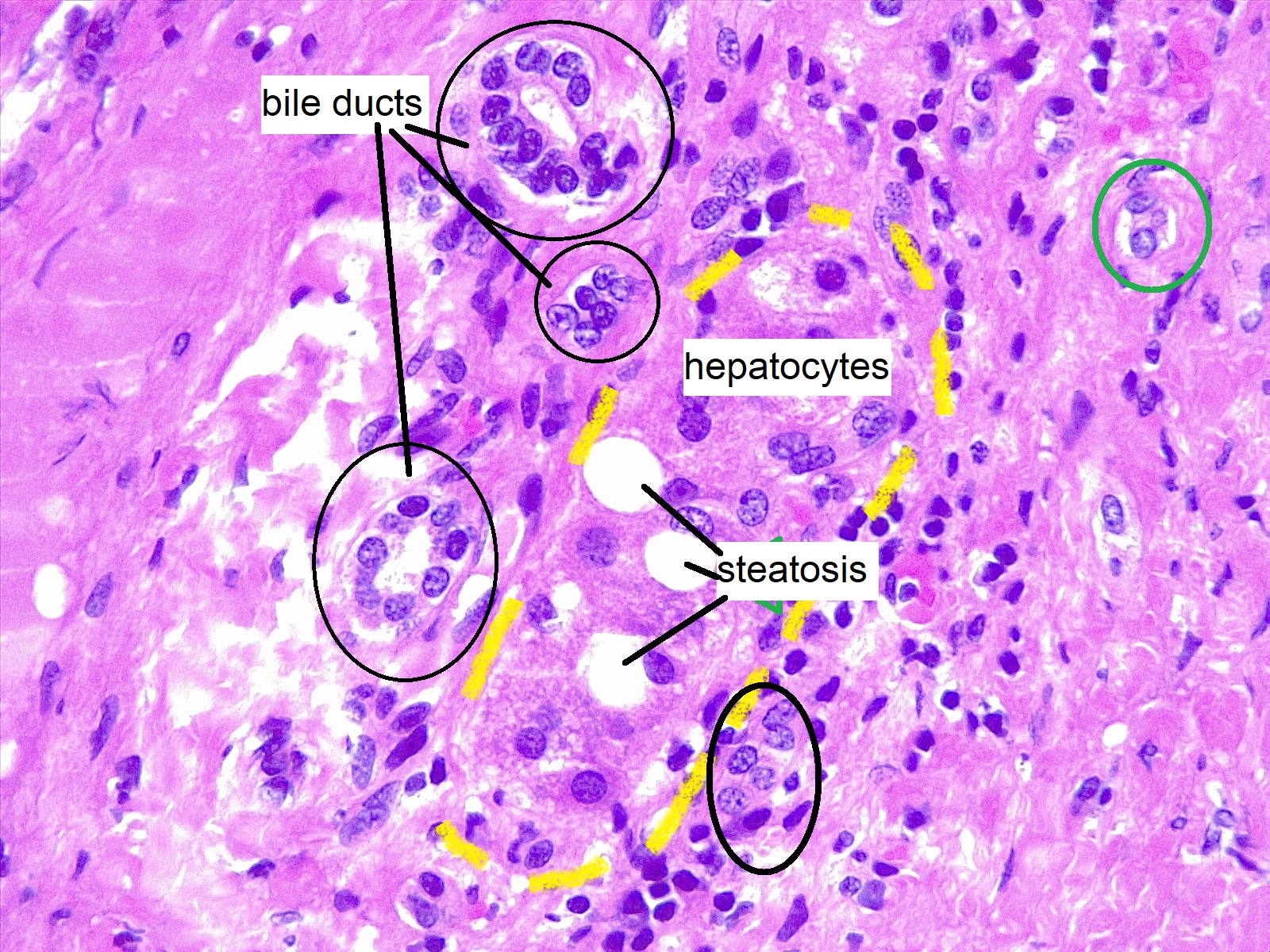
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Fatty liver (hepatic steatosis) is the abnormal accumulation of lipid (predominantly triglycerides) within hepatocytes, visible as clear cytoplasmic vacuoles displacing the nucleus to the periphery. It is the histological manifestation of NAFLD or alcoholic liver disease and may progress through steatohepatitis to cirrhosis.
General / Essential Features
- Macro‑vesicular steatosis: large single fat vacuole displacing nucleus to cell periphery
- Ballooned hepatocytes: swollen, pale, rarefied cytoplasm indicating cell injury
- Dilated central vein
- Micro‑vesicular steatosis (severe cases): multiple small vacuoles, nucleus central
- Perivenular accentuation (alcoholic); pan‑lobular (NAFLD)
- Mallory–Denk bodies (eosinophilic intracytoplasmic inclusions) in NASH
Sites
- Centrilobular (zone 3): alcoholic and NAFLD/NASH — most common pattern
- Periportal (zone 1): malnutrition, pregnancy, toxins
- Pan‑lobular: severe systemic disease
Pathophysiology
Two-hit hypothesis (NAFLD): first hit — lipid accumulation (insulin resistance → increased FFA delivery to liver); second hit — oxidative stress, mitochondrial dysfunction, and inflammatory cytokines (TNF‑α, IL‑6) drive steatohepatitis and fibrosis. Alcohol causes direct mitochondrial toxicity, NAD depletion, and increased fatty acid synthesis.
Etiology
- NAFLD/NASH: obesity, type 2 diabetes, metabolic syndrome — most common
- Alcohol excess: >21 units/week (males), >14 units/week (females)
- Drugs: amiodarone, methotrexate, corticosteroids, tamoxifen, valproate
- Acute fatty liver of pregnancy (AFLP): obstetric emergency
- Reye syndrome, Wilson's disease, starvation/TPN
Clinical Features
- Often asymptomatic — incidental finding on imaging
- Hepatomegaly: smooth, soft liver
- Elevated ALT/AST (AST:ALT <2 in NAFLD; >2 suggests alcohol)
- Fatigue and right upper quadrant discomfort
- NASH may progress: cirrhosis, portal hypertension, HCC
Diagnosis
- Ultrasound: bright (echogenic) liver; sensitivity 60–94%
- Fibroscan (transient elastography): steatosis + fibrosis assessment
- Liver biopsy: gold standard — NAS score for NAFLD (steatosis + ballooning + inflammation)
- LFTs, fasting glucose, lipid profile, HbA1c
Treatment
- Weight loss (>7–10%): most effective intervention for NAFLD
- Alcohol abstinence: essential for alcoholic fatty liver
- Vitamin E: for non‑diabetic NASH (improves NAS score)
- GLP‑1 agonists (semaglutide): emerging evidence for NASH regression
- Liver transplantation: for end‑stage NASH cirrhosis
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test