Adenocarcinoma
Lesson 10 of 15 · Detailed pathology
Points of Recognition
- 1Malignant glandular structures infiltrating stroma
- 2Pleomorphic columnar cells with nuclear hyperchromasia
- 3Intraluminal mucin and necrotic debris
- 4Desmoplastic stromal reaction
- 5Lymphovascular invasion (in advanced cases)
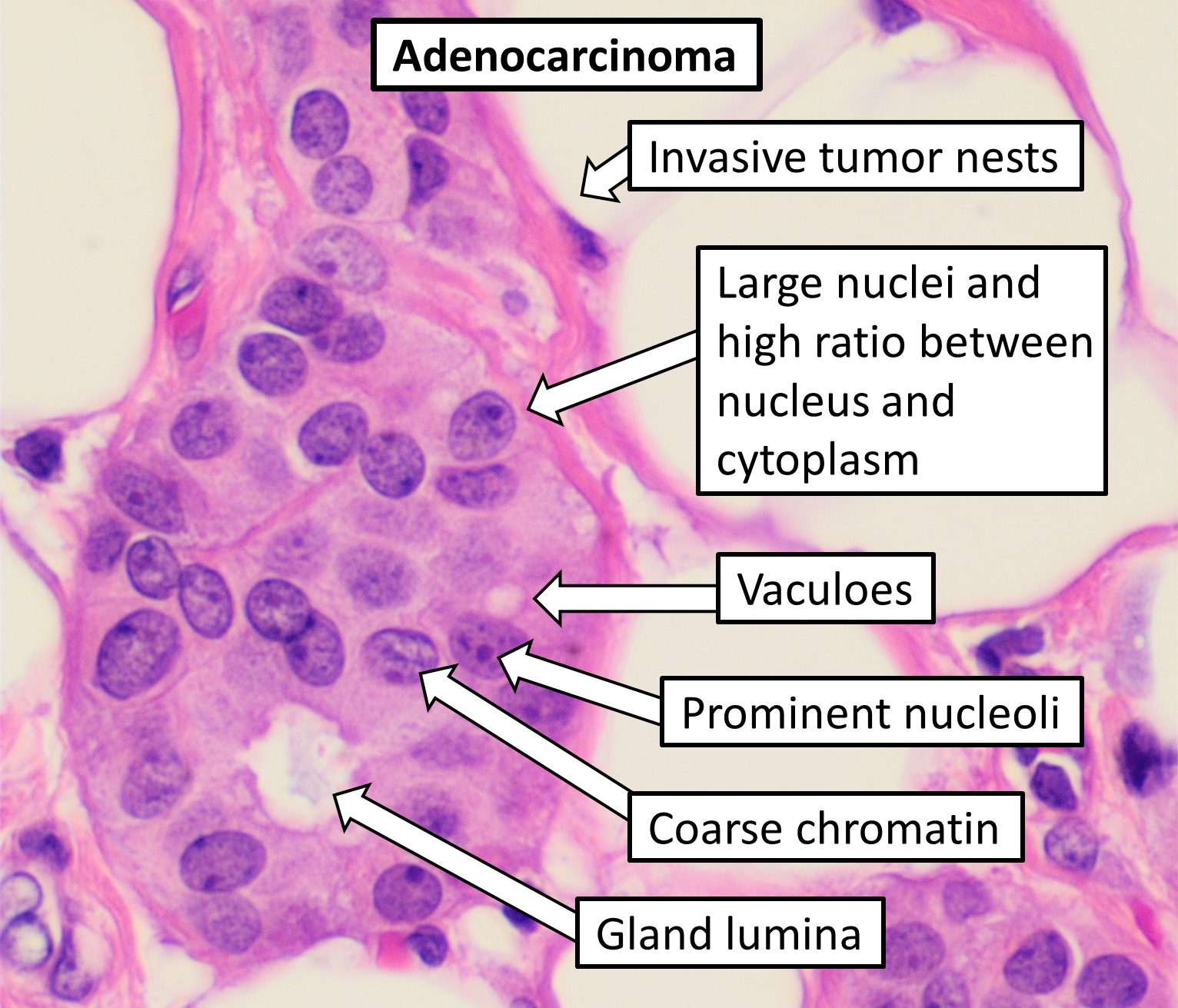
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Adenocarcinoma is a malignant epithelial tumour showing glandular differentiation. Histologically it features irregular malignant glandular structures lined by pleomorphic columnar cells, abundant intraluminal mucin, infiltration through the muscularis mucosae, desmoplastic stromal reaction, and lymphovascular invasion.
General / Essential Features
- Irregular, atypical glandular structures — architectural distortion
- Abundant intraluminal mucin (mucinous variant: >50% mucin pools)
- Cancer cells infiltrating through the muscularis mucosae into submucosa
- Lymphocytic and plasma cell infiltration in the stroma
- Desmoplastic stromal reaction around tumour glands
- Metastasis to regional lymph nodes and distant organs
Sites
- Colorectum: most common adenocarcinoma site in Western countries
- Stomach: intestinal type (H. pylori–driven) and diffuse type (signet-ring cells)
- Lung: peripheral, arising from pneumocytes — most common lung cancer type
- Pancreas: ductal adenocarcinoma — head of pancreas (75%)
- Breast: invasive ductal carcinoma — most common breast malignancy
- Prostate, endometrium, ovary, cervix (endocervical type)
Pathophysiology
Adenocarcinoma follows the adenoma–carcinoma sequence (colon) or Barrett's metaplasia–dysplasia–adenocarcinoma sequence (oesophagus). Driver mutations include KRAS, TP53, SMAD4 (colon); CDH1, RUNX3 (gastric); EGFR, ALK, ROS1 (lung). Invasion is mediated by MMPs and E-cadherin loss (epithelial–mesenchymal transition).
Etiology
- Colonic: adenoma–carcinoma sequence; HNPCC (Lynch syndrome), FAP
- Gastric: H. pylori → chronic gastritis → intestinal metaplasia → carcinoma
- Lung: smoking (though adenocarcinoma is the commonest type in non-smokers)
- Pancreatic: smoking, chronic pancreatitis, hereditary pancreatitis
Clinical Features
- Colorectal: change in bowel habit, rectal bleeding, weight loss, mass per rectum
- Gastric: dysphagia, weight loss, early satiety, Virchow's node
- Lung: haemoptysis, pleural effusion, clubbing
- Pancreatic: painless obstructive jaundice, Courvoisier's sign, steatorrhoea
Diagnosis
- Endoscopy and biopsy: colonoscopy for colorectal, OGD for gastric
- CT/PET-CT: staging and metastasis assessment
- Histopathology: glandular architecture, invasion, desmoplasia
- Molecular profiling: KRAS, EGFR, ALK, HER2, MSI/MMR status
Treatment
- Surgical resection: hemicolectomy, gastrectomy, pneumonectomy, Whipple's
- Adjuvant chemotherapy: FOLFOX (colorectal), FLOT (gastric), carboplatin-paclitaxel (lung)
- Targeted therapy: bevacizumab (anti-VEGF), cetuximab (anti-EGFR), osimertinib (EGFR-mutant lung)
- Immunotherapy: pembrolizumab for MSI-high or PD-L1 positive tumours
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test