Fibroadenoma
Lesson 14 of 15 · Detailed pathology
Points of Recognition
- 1Biphasic proliferation: glands + stroma
- 2Intracanalicular pattern (compressed slits) or pericanalicular (open glands)
- 3Stroma may be myxoid or hyalinised
- 4Well-circumscribed border
- 5Absence of stromal overgrowth or atypia (distinguishes from phyllodes)
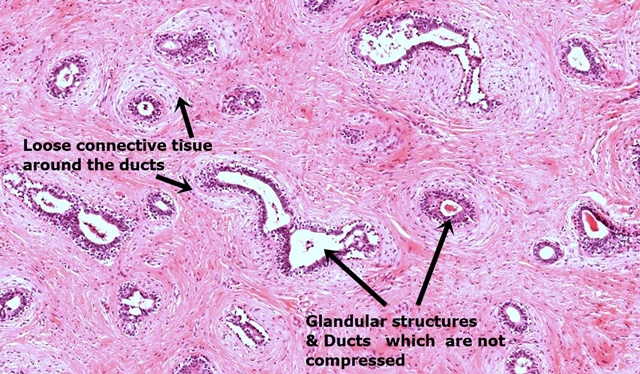
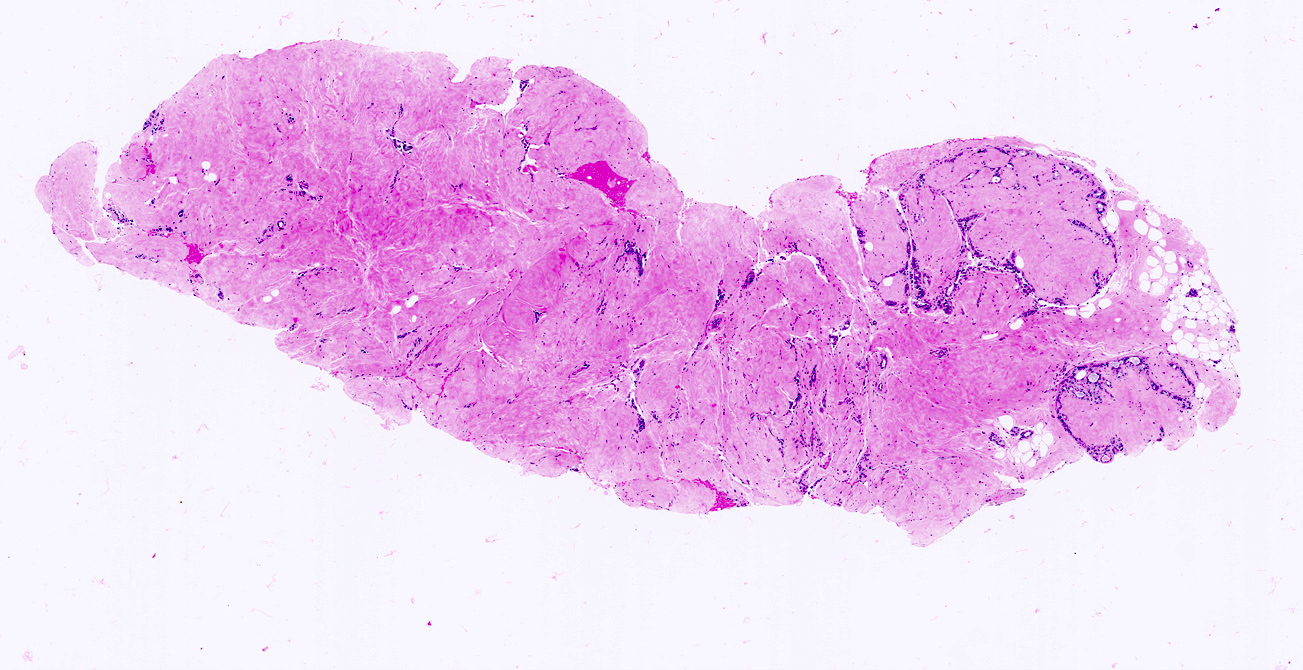
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Fibroadenoma is the most common benign breast tumour in women under 30. It is a biphasic tumour composed of epithelial (acinar and ductal) and stromal (fibroblastic) elements. Two histological patterns exist: pericanalicular (fibrous stroma encircles rounded acini) and intracanalicular (fibrous stroma compresses ducts into elongated slit-like clefts).
General / Essential Features
- Biphasic tumour: epithelial + fibroblastic stromal components
- Small acini and duct-like structures resembling normal breast tissue
- Fibrous stroma arranged around and between acini
- Epithelial clefts (slit-like) formed by fibrous compression — intracanalicular pattern
- Benign epithelium: regular nuclei, no atypia, no mitoses
- Well-circumscribed; usually encapsulated
Sites
- Upper outer quadrant of the breast (most common quadrant for all breast lesions)
- Typically solitary; multiple in 10–15% (giant fibroadenoma in juveniles)
- No specific lobar distribution
Pathophysiology
Fibroadenomas arise from the terminal duct–lobular unit (TDLU). Oestrogenic stimulation during reproductive years drives growth; lesions often enlarge during pregnancy and regress post-menopause. MED12 mutations (as in uterine fibroids) have been identified. Giant juvenile fibroadenoma occurs in adolescents and can be rapidly growing.
Etiology
- Hormonal: oestrogen-sensitive — common in reproductive years
- MED12 somatic mutations
- Black women of Caribbean or African descent: higher incidence of multiple/giant fibroadenomas
- Cyclosporine use after renal transplant — associated with giant fibroadenoma
Clinical Features
- Smooth, mobile, well-defined, non-tender breast lump ('breast mouse')
- Usually 1–3 cm; may be multiple
- No skin changes, no nipple discharge
- Triple assessment: clinical + ultrasound + FNAC/core biopsy
- Malignant transformation extremely rare (<0.1%)
Diagnosis
- Ultrasound: well-defined, homogeneous, hypoechoic lesion with gentle lobulations
- FNAC / core biopsy: confirms benign biphasic histology
- Mammography: in women over 35 — calcified fibroadenoma ('popcorn' calcification)
- MRI: for multiple lesions or in high-risk patients
Treatment
- Conservative management for lesions <3 cm with confirmed benign histology
- Surgical excision: for >3 cm, growing, or patient anxiety
- Vacuum-assisted biopsy excision: ultrasound-guided, no scar
- Annual review: to monitor size and exclude interval change
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test