Peptic Ulcer
Lesson 4 of 15 · Detailed pathology
Points of Recognition
- 1Fibrinoid necrosis at the surface of ulcer crater
- 2Granulation tissue beneath necrotic zone
- 3Fibrosis and chronic inflammation at base
- 4Thrombosed or eroded vessels in the ulcer floor
- 5Intestinal metaplasia at ulcer edge (in stomach)
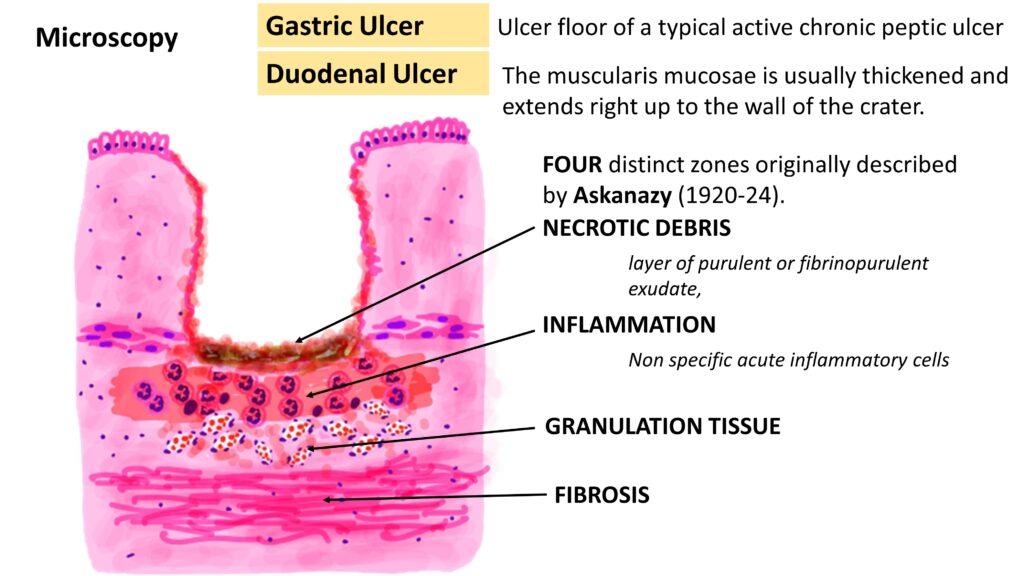
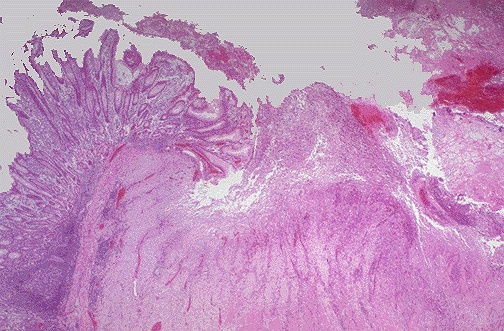
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Peptic ulcer is a full-thickness mucosal defect that penetrates through the muscularis mucosae, occurring in areas exposed to acid-pepsin digestion. Classic sites are the gastric antrum and the first part of the duodenum (duodenal ulcer). H. pylori and NSAIDs are the two principal aetiological factors.
General / Essential Features
- Sharply demarcated, punched-out ulcer edges (unlike malignant ulcer with heaped-up edges)
- Degeneration / necrosis of mucosal epithelium at ulcer base
- Four-zone histology: fibrinous exudate → coagulation necrosis → granulation tissue → fibrous scar
- Blood vessels at the ulcer base — erosion causes haemorrhage
- Inflammatory cells: lymphocytes, plasma cells, eosinophils in ulcer margin
- Perforation of ulcer leads to acute peritonitis
Sites
- Duodenal ulcer (DU): anterior wall of first part of duodenum — most common
- Gastric ulcer (GU): lesser curvature of the antrum
- Stomal ulcer: at gastroenterostomy anastomosis
- Zollinger–Ellison syndrome: multiple ulcers in atypical sites (jejunum)
Pathophysiology
Imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and defensive factors (mucus, bicarbonate, prostaglandins, epithelial renewal). NSAIDs inhibit COX-1, reducing mucoprotective prostaglandin synthesis. H. pylori undermines the mucus layer and impairs bicarbonate secretion. Acid contact with exposed lamina propria causes progressive tissue necrosis.
Etiology
- H. pylori infection: ~80% of duodenal ulcers, ~70% of gastric ulcers
- NSAIDs / aspirin: second commonest cause — especially in elderly
- Zollinger–Ellison syndrome: gastrinoma causing massive acid hypersecretion
- Stress ulcers: Curling (burns), Cushing (raised ICP) ulcers
- Smoking: delays healing, increases recurrence
Clinical Features
- DU: epigastric pain relieved by food and antacids; nocturnal waking pain
- GU: epigastric pain precipitated or worsened by food
- Haematemesis or melaena (bleeding — most common complication)
- Sudden severe abdominal pain: perforation → peritonitis
- Pyloric obstruction: projectile vomiting, succussion splash
Diagnosis
- Upper GI endoscopy (OGD): visualises ulcer; biopsy GU to exclude malignancy
- H. pylori testing: CLO test, breath test, stool antigen
- Barium meal: filling defect (rarely used now)
- Fasting serum gastrin: if ZES suspected (>1000 pg/mL diagnostic)
Treatment
- H. pylori eradication: 7-day triple therapy (PPI + amoxicillin + clarithromycin)
- PPI (omeprazole 20 mg BD) for 4–8 weeks
- Stop NSAIDs; use selective COX-2 inhibitors with PPI if unavoidable
- Emergency: endoscopic haemostasis (adrenaline injection, clips) for bleeding
- Surgery: rarely — perforated ulcer repair (Graham patch), vagotomy
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test