Squamous Cell Carcinoma
Lesson 8 of 15 · Detailed pathology
Points of Recognition
- 1Keratin pearls (concentric whorls of keratin)
- 2Intercellular bridges (prickles) between cells
- 3Invasion of dermis/submucosa by malignant squamous nests
- 4Nuclear atypia and atypical mitoses
- 5Individual cell keratinisation (dyskeratosis)
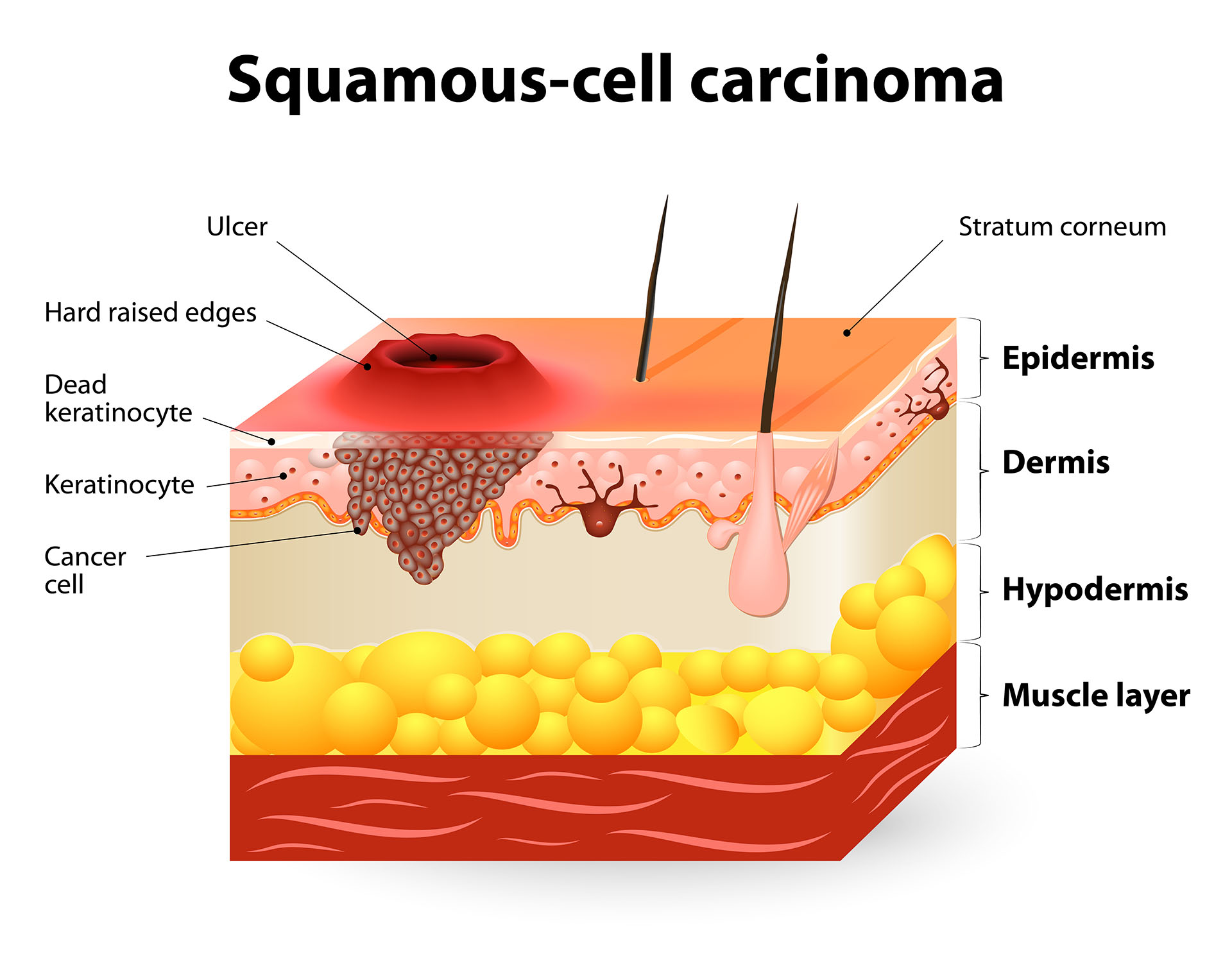
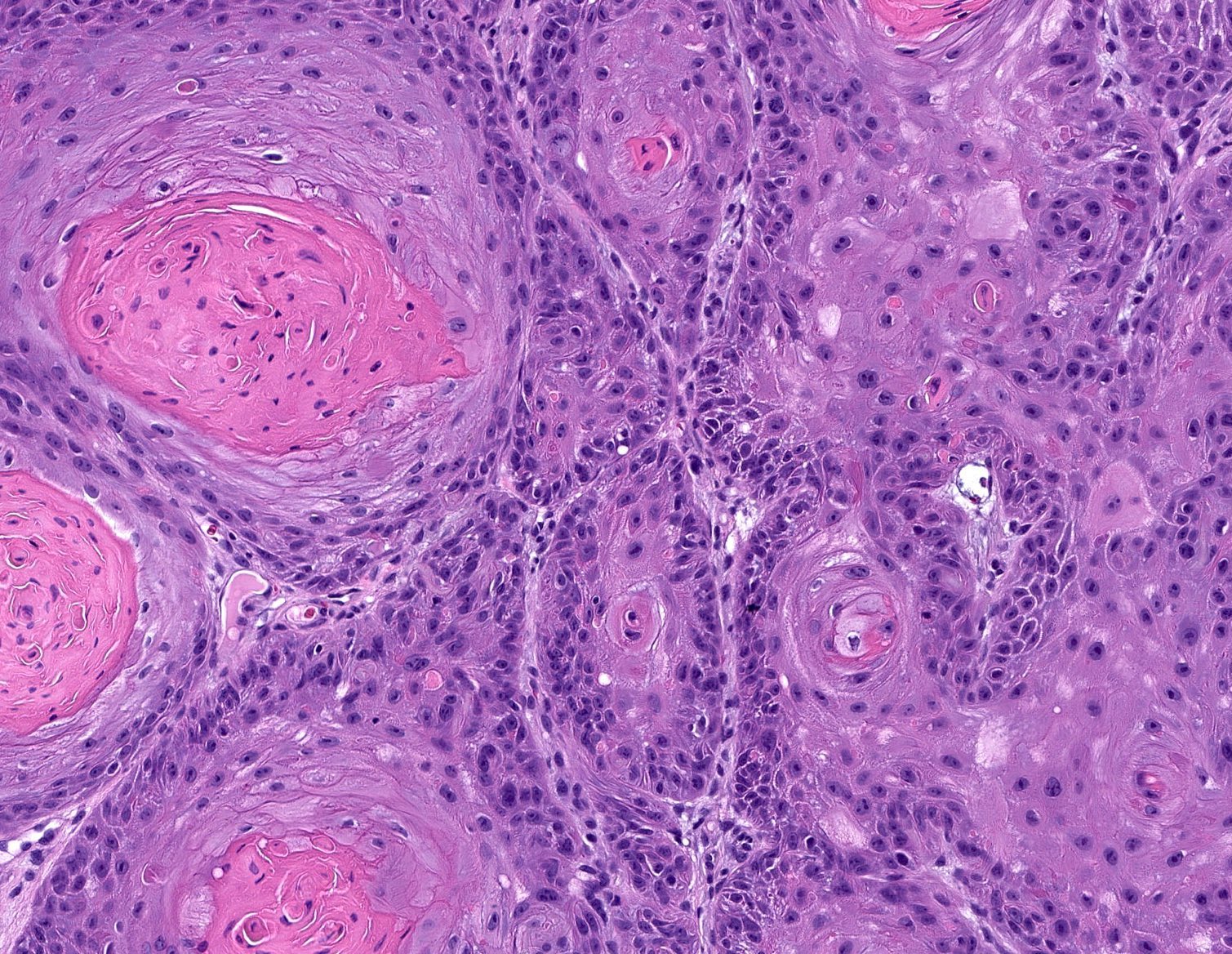
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Squamous cell carcinoma (SCC) is a malignant tumour of squamous epithelial cells, characterised by large polygonal cells with eosinophilic cytoplasm, intercellular desmosomes (prickle cells), keratin pearl formation, and stromal invasion. It arises from stratified squamous epithelium or from squamous metaplasia.
General / Essential Features
- Large polygonal cells with abundant eosinophilic cytoplasm
- Concentric whorls of keratinised cells forming keratin pearls
- Desmosomal connections (intercellular bridges) between adjacent cells
- Tumour cell infiltration into the underlying stroma, breaching the basement membrane
- Lymphocytic infiltrate ± plasma cells in the stroma (host response)
- Nuclear pleomorphism, hyperchromasia, and abnormal mitoses
Sites
- Skin: sun-exposed areas, particularly head, neck, dorsal hands
- Oral cavity: tongue, floor of mouth (smoking + alcohol)
- Oesophagus: middle and lower third
- Lung: hilar, central, arising from bronchial epithelium (smoking)
- Cervix: squamocolumnar junction (HPV 16/18)
- Penis, vulva, anal canal
Pathophysiology
UV radiation, tobacco carcinogens, or HPV oncoproteins (E6/E7) disrupt p53 and Rb tumour-suppressor pathways, leading to uncontrolled proliferation of squamous cells. Cells lose polarity, invade the stroma, and produce dyskeratotic cells. Desmoplastic reaction around tumour nests provides structural support for invasion and metastasis.
Etiology
- UV radiation (skin SCC): UVB-induced p53 mutation
- Smoking and alcohol (oral, oesophageal, lung SCC)
- HPV 16 and 18: cervical, oropharyngeal, and anogenital SCC
- Chronic irritation: Marjolin's ulcer (SCC arising in chronic wounds/scars)
- Immunosuppression: organ transplant recipients — greatly elevated risk
Clinical Features
- Skin: indurated, keratotic nodule or ulcer with everted edges
- Oral: non-healing ulcer, leukoplakia, erythroplakia
- Lung: haemoptysis, recurrent pneumonia, Pancoast syndrome
- Cervix: post-coital bleeding, foul-smelling discharge
- Metastasis: regional lymph nodes (hard, non-tender), distant organs
Diagnosis
- Biopsy and histopathology: gold standard
- Histology: keratin pearls, desmosomes, stromal invasion
- HPV testing (cervical): PCR-based genotyping
- Staging CT/PET-CT: lymph node and distant metastasis assessment
Treatment
- Surgical excision with clear margins: primary treatment for localised SCC
- Mohs micrographic surgery: for facial/skin SCC — margin controlled
- Radiotherapy: for non-surgical candidates or adjuvant post-excision
- Chemoradiation (cisplatin-based): locally advanced disease
- Immune checkpoint inhibitors (pembrolizumab): metastatic/recurrent SCC
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test