Chronic Cholecystitis
Lesson 2 of 15 · Detailed pathology
Points of Recognition
- 1Rokitansky–Aschoff sinuses (epithelial herniations through muscularis)
- 2Chronic inflammatory infiltrate (lymphocytes, plasma cells)
- 3Fibrosis and thickening of gallbladder wall
- 4Associated gallstones in most cases
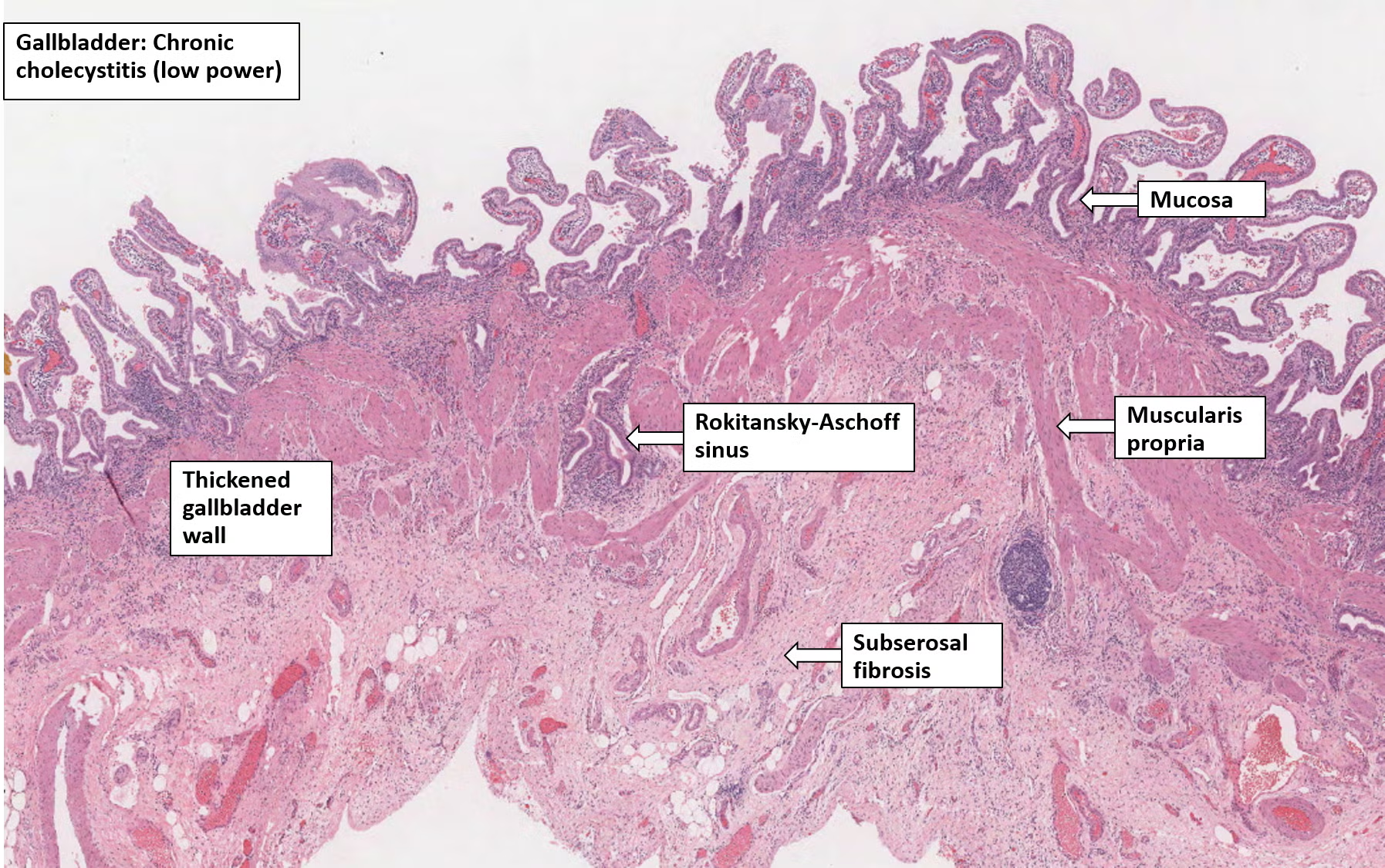
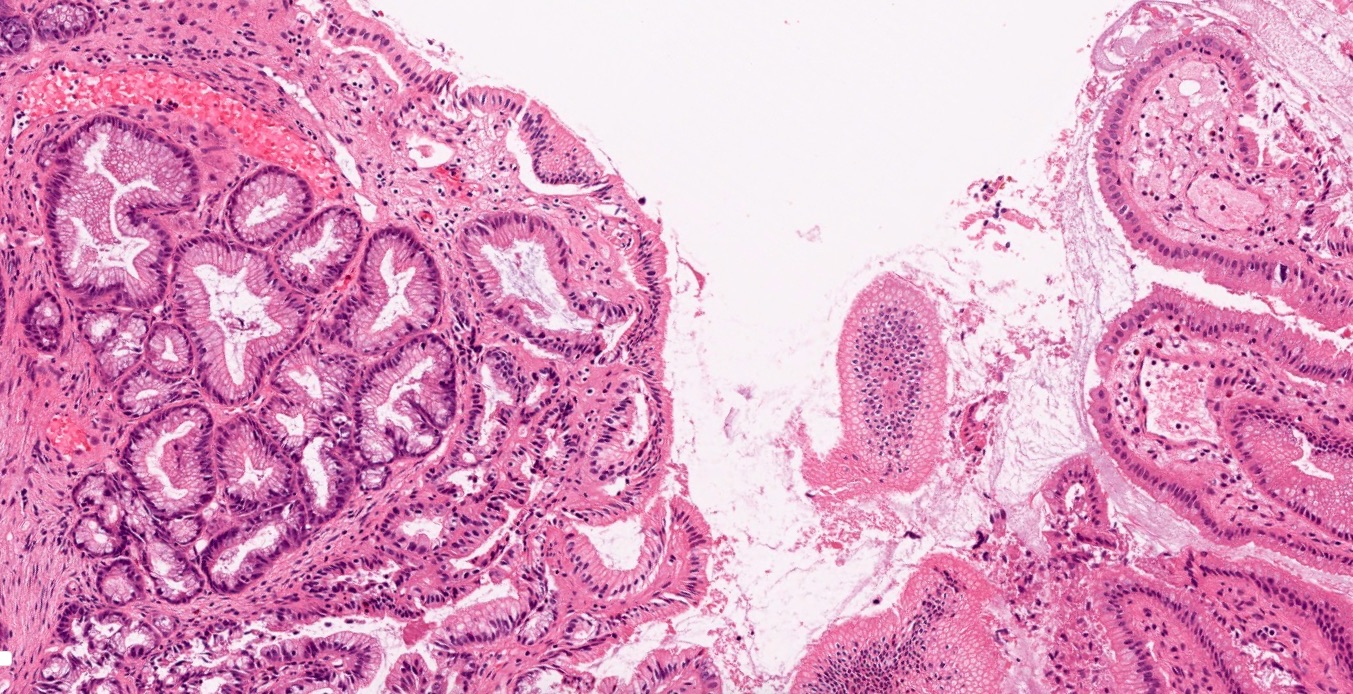
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Chronic cholecystitis is chronic, recurrent low-grade inflammation of the gallbladder, almost always associated with cholelithiasis (gallstones). Repeated bouts of obstruction and mild inflammation lead to fibrosis, wall thickening, and the formation of pathognomonic Rokitansky–Aschoff sinuses.
General / Essential Features
- Rokitansky–Aschoff sinuses (RAS): epithelium-lined crypts herniating through the muscularis
- Mononuclear inflammatory infiltrate (lymphocytes, plasma cells) in lamina propria
- Sub-epithelial and sub-serosal fibrosis causing gallbladder shrinkage
- Hypertrophy of the muscularis propria
- Cholesterol clefts or calcium deposits may be present
- Mucosal folds may be flattened or atrophied
Sites
- Gallbladder — body and fundus most commonly affected
- Associated with gallstones in >90% of cases
- Porcelain gallbladder: dystrophic calcification of the wall (rare)
Pathophysiology
Repeated mechanical irritation and intermittent obstruction by gallstones activate a chronic inflammatory cascade. Persistent inflammation leads to mucosal metaplasia, fibrosis, and muscle hypertrophy. Increased intraluminal pressure forces epithelium into the wall, creating RAS. Shrinkage and scarring impair gallbladder contractility.
Etiology
- Cholelithiasis (gallstones) — present in >90%
- Acalculous chronic cholecystitis — rare, secondary to ischaemia or infection
- Risk factors: female, fat, forty, fertile (5 Fs)
- Salmonella typhi chronic carrier state can cause cholecystitis
Clinical Features
- Recurrent right upper quadrant or epigastric pain (biliary colic)
- Nausea and fat intolerance
- Pain precipitated by fatty meals (cholecystokinin release)
- Murphy's sign positive on deep palpation
- Jaundice if common bile duct obstructed (Mirizzi syndrome)
Diagnosis
- Ultrasound: gallstones, thickened gallbladder wall (>3 mm), pericholecystic fluid
- HIDA scan: reduced gallbladder ejection fraction (<35%)
- CT/MRCP: complications and anatomy
- Histopathology post-cholecystectomy: confirms chronic inflammation and RAS
Treatment
- Elective laparoscopic cholecystectomy — definitive treatment
- Low-fat diet for symptomatic relief pre-operatively
- ERCP with stone extraction if choledocholithiasis present
- Ursodeoxycholic acid (UDCA) for dissolution in non-surgical candidates
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test