Carcinoma In Situ
Lesson 15 of 15 · Detailed pathology
Points of Recognition
- 1Full-thickness loss of epithelial maturation (CIN 3)
- 2Intact basement membrane – no stromal invasion
- 3Increased mitotic figures, including at upper levels
- 4Nuclear atypia (pleomorphism, hyperchromasia)
- 5May involve endocervical crypts (SMILE)
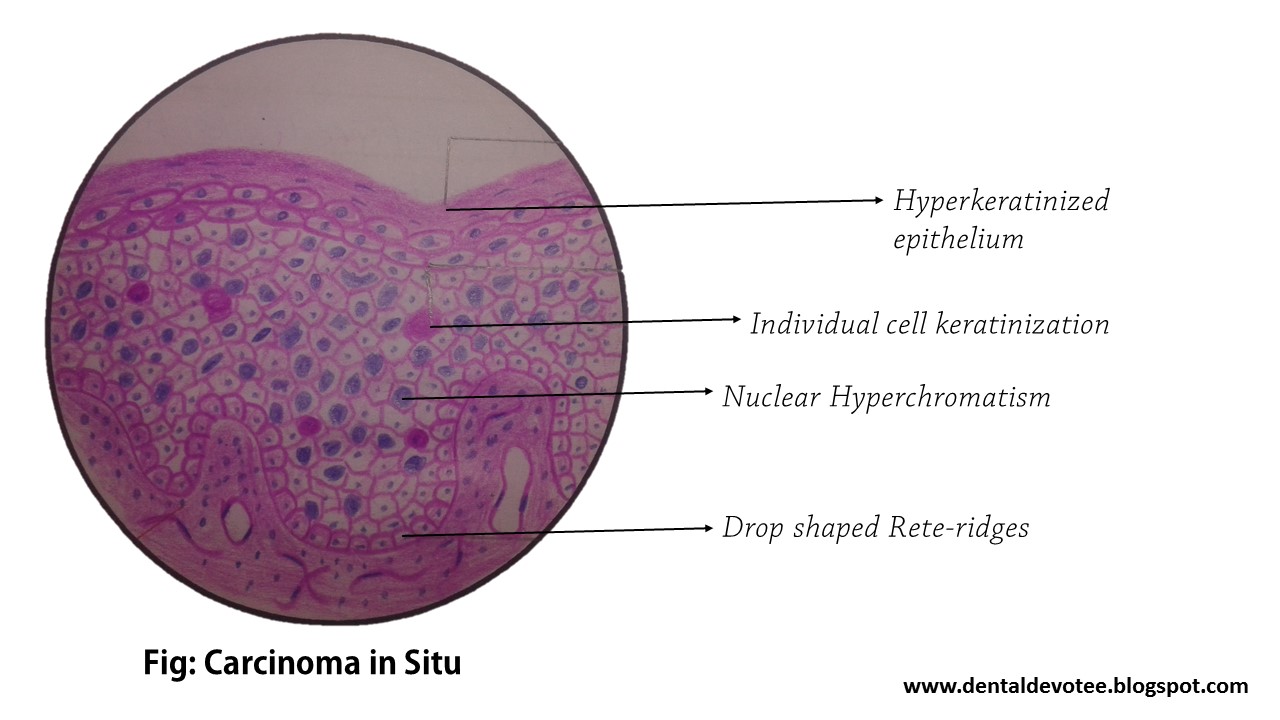
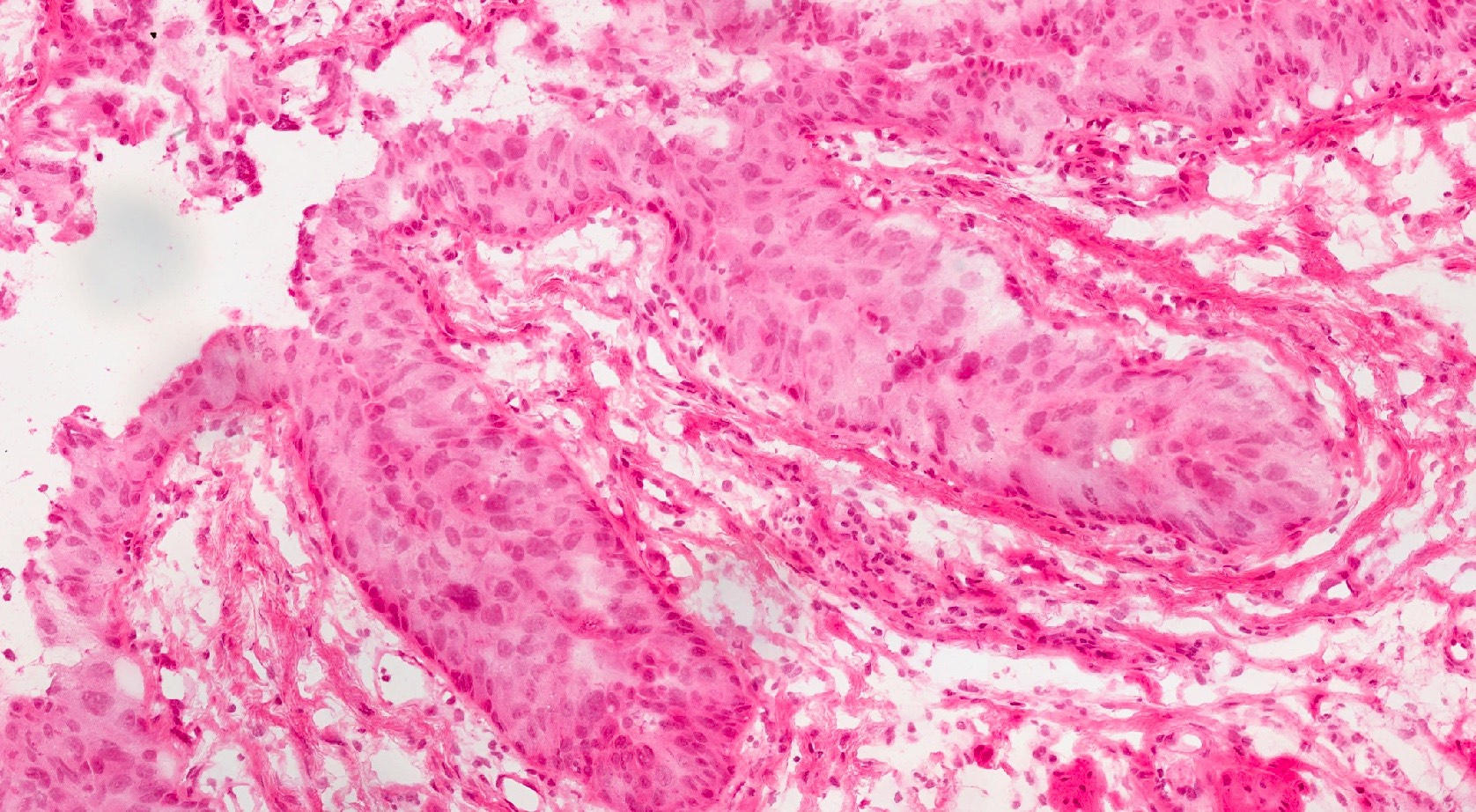
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Carcinoma in situ (CIS) is full-thickness neoplastic transformation of the squamous epithelium without stromal invasion — equivalent to CIN 3 / high-grade squamous intraepithelial lesion (HSIL). The SMILE (Stratified Mucin-secreting Intraepithelial Lesion) variant involves endocervical crypts with polyhedral undifferentiated cells and mucinous cytoplasm.
General / Essential Features
- SMILE: Stratified Mucin-secreting Intraepithelial Lesion — endocervical crypt involvement
- Polyhedral columnar cells with eosinophilic to mucinous cytoplasm
- No clear stratification — cells are undifferentiated throughout full thickness
- Increased mitotic activity at all levels of the epithelium
- Abnormal cells filling the endocervical crypts without invasion
- Intact basement membrane — no stromal breach (in situ by definition)
Sites
- Squamocolumnar junction (transformation zone) of the cervix
- Endocervical crypts involved in CIS/SMILE
- May extend into vaginal fornices (VAIN) or endocervical canal
Pathophysiology
HPV 16 and 18 oncoproteins E6 (degrades p53) and E7 (inactivates Rb) drive uncontrolled cell cycle entry and genomic instability. Full-thickness loss of maturation and polarity results. Integration of HPV genome into the host chromosome upregulates E6/E7 expression. Without treatment, 30–70% of CIN 3 progresses to invasive carcinoma over 10–20 years.
Etiology
- HPV 16 (most oncogenic): associated with squamous CIS
- HPV 18: more associated with adenocarcinoma in situ
- Risk factors: early sexual activity, multiple partners, smoking, immunosuppression
- Previous CIN 1/2 progression
- HIV infection: greatly elevated risk
Clinical Features
- Usually asymptomatic — detected on cervical screening (Pap smear / liquid-based cytology)
- Post-coital bleeding if associated with erosion
- Colposcopy: acetowhite areas, punctation, mosaicism at transformation zone
- High-grade changes on cervical smear (HSIL / CIN 3 cytology)
- Progression to invasive cancer if untreated
Diagnosis
- Cervical smear (LBC): HSIL cells
- HPV genotyping: high-risk HPV 16/18
- Colposcopy and targeted biopsy: gold standard
- Histopathology: full-thickness dysplasia, SMILE, intact BM
- Large loop excision of the transformation zone (LLETZ): diagnostic and therapeutic
Treatment
- LLETZ (LEEP): electrosurgical loop excision — first-line treatment for CIN 3 / CIS
- Cone biopsy: cold knife cone — for glandular lesions or depth needed
- Cryotherapy / laser ablation: for carefully selected CIN 2–3
- Hysterectomy: for recurrent CIS or completed family
- HPV vaccination (Gardasil-9): primary prevention against HPV 16/18
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test