Benign Prostatic Hyperplasia
Lesson 13 of 15 · Detailed pathology
Points of Recognition
- 1Nodular hyperplasia of glands and stroma in transitional zone
- 2Cystically dilated glands with papillary infoldings
- 3Double-layered epithelium (basal + luminal)
- 4Corpora amylacea in gland lumens
- 5Stromal component: smooth muscle and fibrous tissue
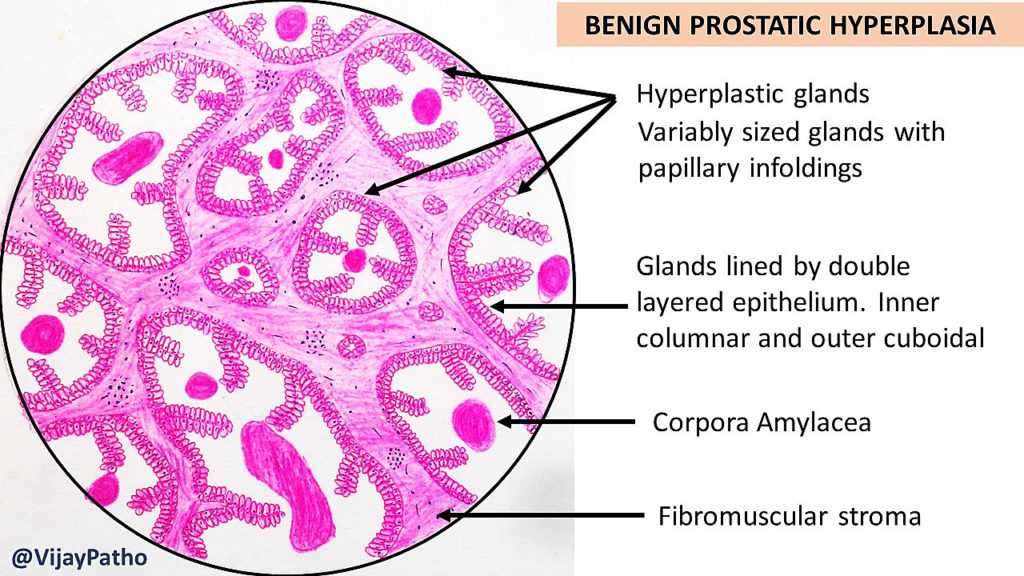
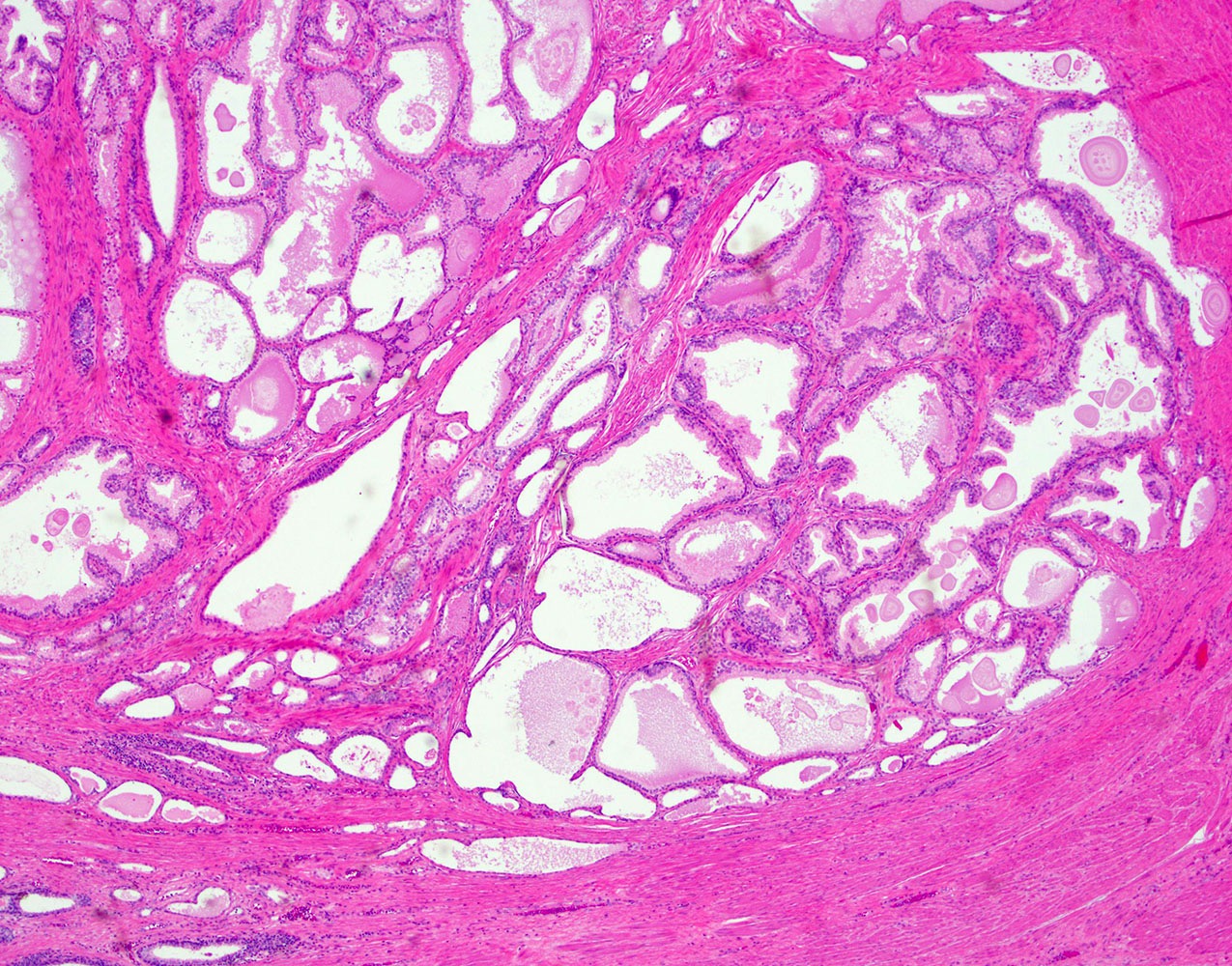
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Benign Prostatic Hyperplasia (BPH) is non-neoplastic proliferation of both glandular and stromal elements in the periurethral transitional zone of the prostate, driven by dihydrotestosterone (DHT). Histologically it features enlarged glands with papillary projections lined by double-layer epithelium (inner columnar + outer cuboidal basal cells) and cystic dilation.
General / Essential Features
- Cystic glandular spaces with papillary projections into the lumen
- Double-layer epithelium: inner tall columnar secretory cells + outer cuboidal basal cells
- Corpora amylacea: laminated eosinophilic concretions in gland lumens
- Increased fibromuscular stromal component
- Secondary bladder changes: detrusor hypertrophy, diverticulum
- No invasion, no significant atypia — distinguishes from carcinoma
Sites
- Transitional (periurethral) zone of the prostate — exclusive site of BPH
- Peripheral zone: site of most prostate carcinomas (not BPH)
- Enlargement compresses the prostatic urethra causing LUTS
Pathophysiology
Testosterone is converted to DHT by 5α-reductase in stromal cells. DHT binds androgen receptors and promotes epithelial and stromal proliferation. Relative androgen/oestrogen imbalance with ageing amplifies this effect. Mechanical obstruction of the urethra causes LUTS; chronic retention leads to hydronephrosis.
Etiology
- Ageing: prevalence increases from 8% at 31–40 years to 80% by age 80
- Androgens: DHT via 5α-reductase is the key driver
- Oestrogen: relative increase with ageing may sensitise stroma
- Genetic: strong familial component; multiple susceptibility loci
Clinical Features
- Lower urinary tract symptoms (LUTS): hesitancy, poor stream, terminal dribbling
- Storage symptoms: frequency, urgency, nocturia
- Acute urinary retention: precipitated by constipation, cold, anticholinergics
- Digital rectal exam: symmetrically enlarged, smooth, firm, non-tender prostate
- Elevated PSA (but lower density than in carcinoma)
Diagnosis
- IPSS score: International Prostate Symptom Score — severity assessment
- Uroflowmetry: reduced peak flow rate (<10 mL/s)
- Post-void residual volume (PVRV): ultrasound guided
- PSA: to exclude carcinoma
- Cystoscopy / TRUS biopsy if PSA elevated or suspicious features
Treatment
- Alpha-1 blockers (tamsulosin, alfuzosin): relax smooth muscle — first line
- 5α-reductase inhibitors (finasteride, dutasteride): shrink gland — for large glands
- Combination therapy: alpha-blocker + 5-ARI for moderate-severe symptoms
- TURP (transurethral resection of prostate): gold-standard surgical treatment
- Laser prostatectomy (HoLEP), UroLift, Rezum: minimally invasive alternatives
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test