Hodgkin's Disease
Lesson 9 of 15 · Detailed pathology
Points of Recognition
- 1Reed‑Sternberg cells (binucleated, owl‑eye nucleoli)
- 2Mixed inflammatory background (lymphocytes, eosinophils, plasma cells)
- 3CD15+, CD30+, CD45− immunophenotype
- 4Nodular sclerosis subtype with collagen bands
- 5EBV positivity in ~40% (LMP1+)
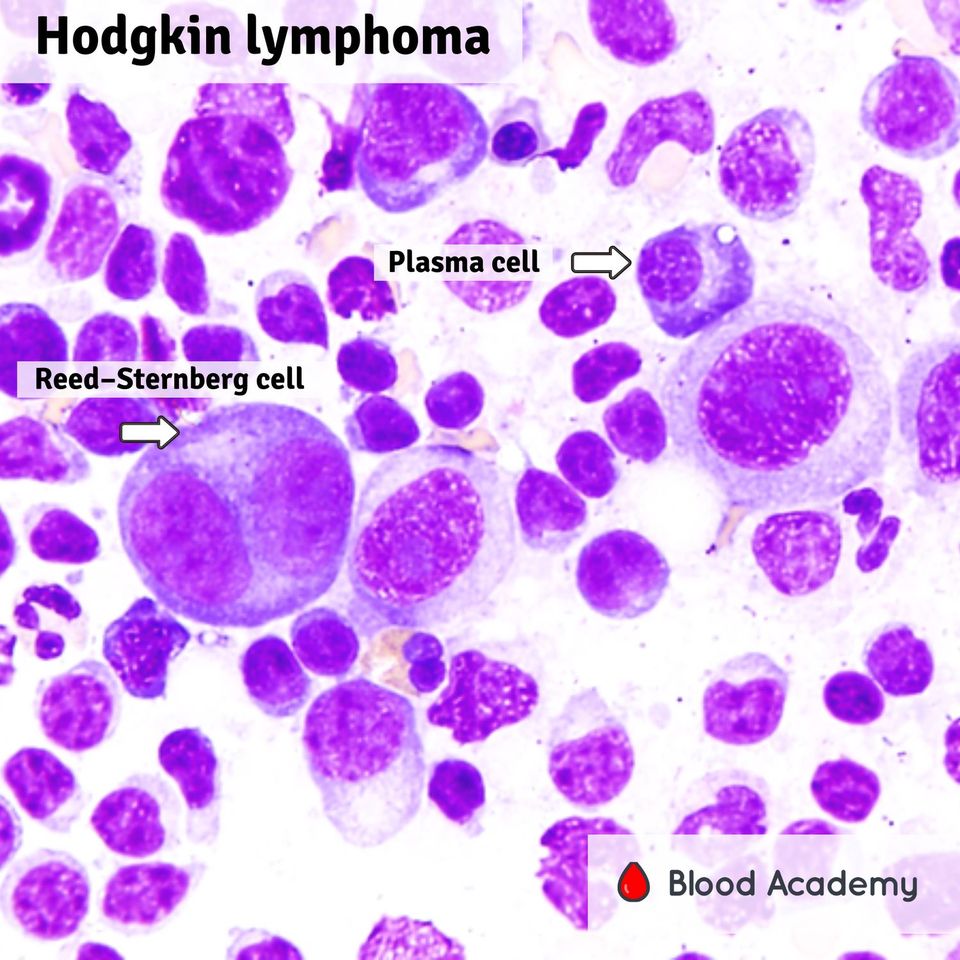
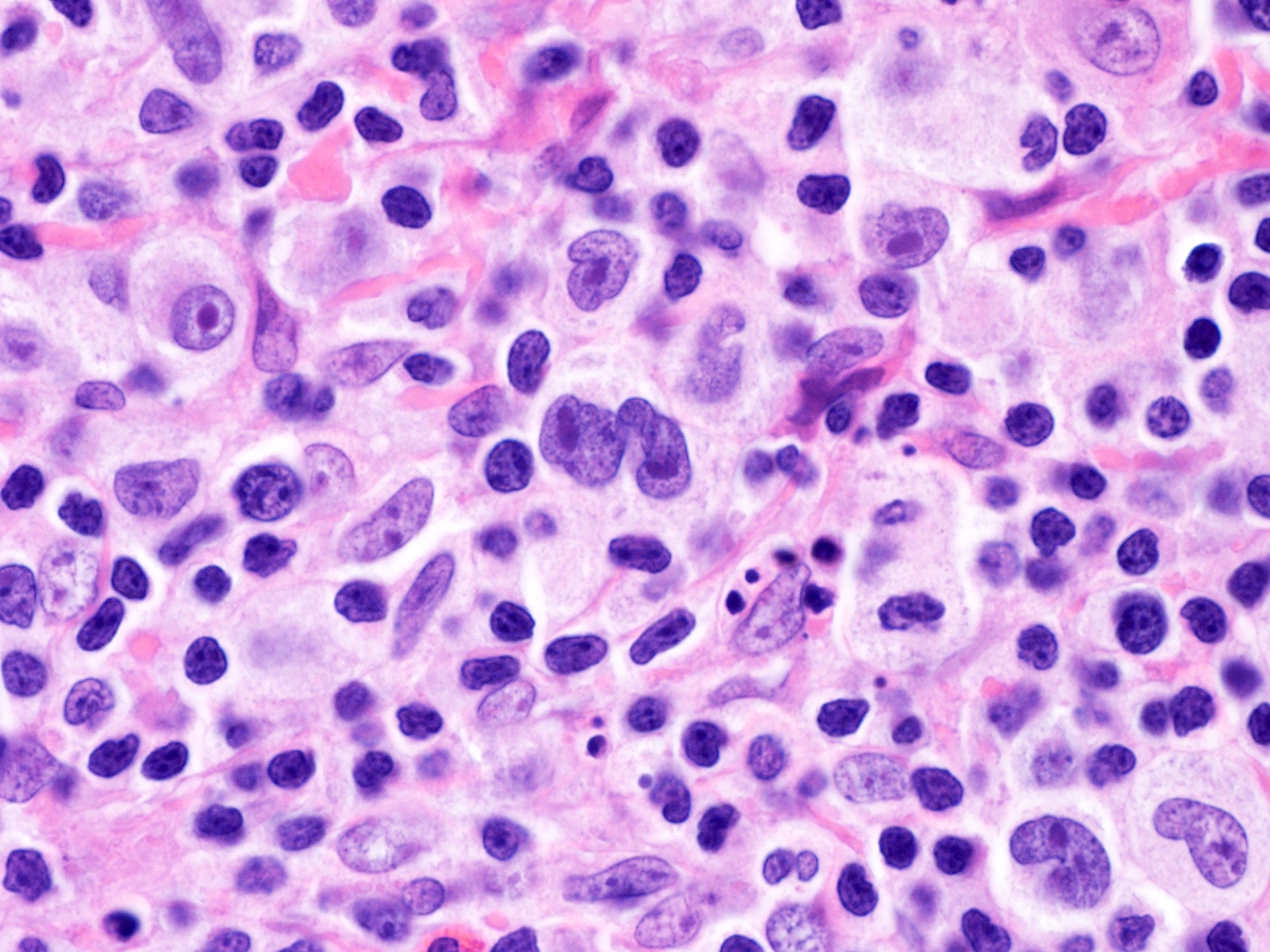
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Hodgkin's lymphoma (Hodgkin's disease) is a B-cell lymphoid malignancy characterised by the presence of Reed–Sternberg (RS) cells — large binucleated or multinucleated cells with prominent eosinophilic 'owl-eye' nucleoli — set against a reactive inflammatory background of lymphocytes, eosinophils, neutrophils, and plasma cells.
General / Essential Features
- Reed–Sternberg cells: large binucleated / multinucleated cells — pathognomonic
- Prominent eosinophilic 'owl-eye' nucleolus in each RS cell nucleus
- Abundant pale eosinophilic cytoplasm in RS cells
- Derived from germinal-centre B-cells (CD15+, CD30+, CD45−)
- Mixed inflammatory background: lymphocytes, eosinophils, plasma cells, neutrophils
- Nodular sclerosis subtype: broad collagen bands dividing lymph node into nodules
Sites
- Cervical and supraclavicular lymph nodes — most common presentation
- Mediastinal lymphadenopathy: nodular sclerosis type (especially young women)
- Axillary and inguinal nodes (less common)
- Spreads in contiguous nodal fashion (unlike NHL)
- Ann Arbor staging: I–IV based on nodal and extranodal involvement
Pathophysiology
RS cells are clonally derived from germinal-centre B-cells that have lost their B-cell programme (loss of PAX5, BCL6 expression but retained CD30, CD15). They secrete IL-13, IL-5, and eotaxin, recruiting eosinophils and creating a tolerogenic microenvironment. EBV latent membrane protein (LMP1) mimics CD40 signalling and is implicated in pathogenesis.
Etiology
- EBV association: LMP1 drives NFκB activation — present in ~40% of cases
- Immunosuppression: HIV-associated Hodgkin's lymphoma
- Genetic predisposition: first-degree relatives, monozygotic twins
- Bimodal age distribution: young adults (15–34) and older adults (>55)
Clinical Features
- Painless cervical lymphadenopathy — most common presentation
- B symptoms: fever, drenching night sweats, weight loss >10% over 6 months
- Mediastinal mass: cough, dyspnoea, SVC syndrome
- Alcohol-induced lymph node pain (pathognomonic)
- Pruritus — generalised
Diagnosis
- Excisional lymph node biopsy: required for subtype classification
- Histopathology + IHC: CD15+, CD30+, CD45−, PAX5 dim
- CT chest/abdomen/pelvis: staging
- PET-CT: gold standard for staging and response assessment
- Bone marrow biopsy: for stage III/IV disease
Treatment
- Early stage (I–II): ABVD chemotherapy × 2–4 cycles ± radiotherapy
- Advanced stage (III–IV): ABVD × 6 cycles or escalated BEACOPP
- PET-adapted therapy: de-escalation in PET-negative responders
- Relapsed/refractory: BV-based salvage + autologous stem cell transplant
- Brentuximab vedotin (anti-CD30): for relapsed HL
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test