🍽️
Pathology Lesson · GI Pathology
Gastritis
Lesson 3 of 15 · Detailed pathology
PathologyGI Pathology
Points of Recognition
- 1Lymphoplasmacytic infiltrate in lamina propria
- 2Neutrophil infiltration (activity) in pit epithelium (H. pylori)
- 3Glandular atrophy and intestinal metaplasia in chronic cases
- 4H. pylori organisms on special stains (Giemsa)
- 5Lymphoid follicles (especially in H. pylori)
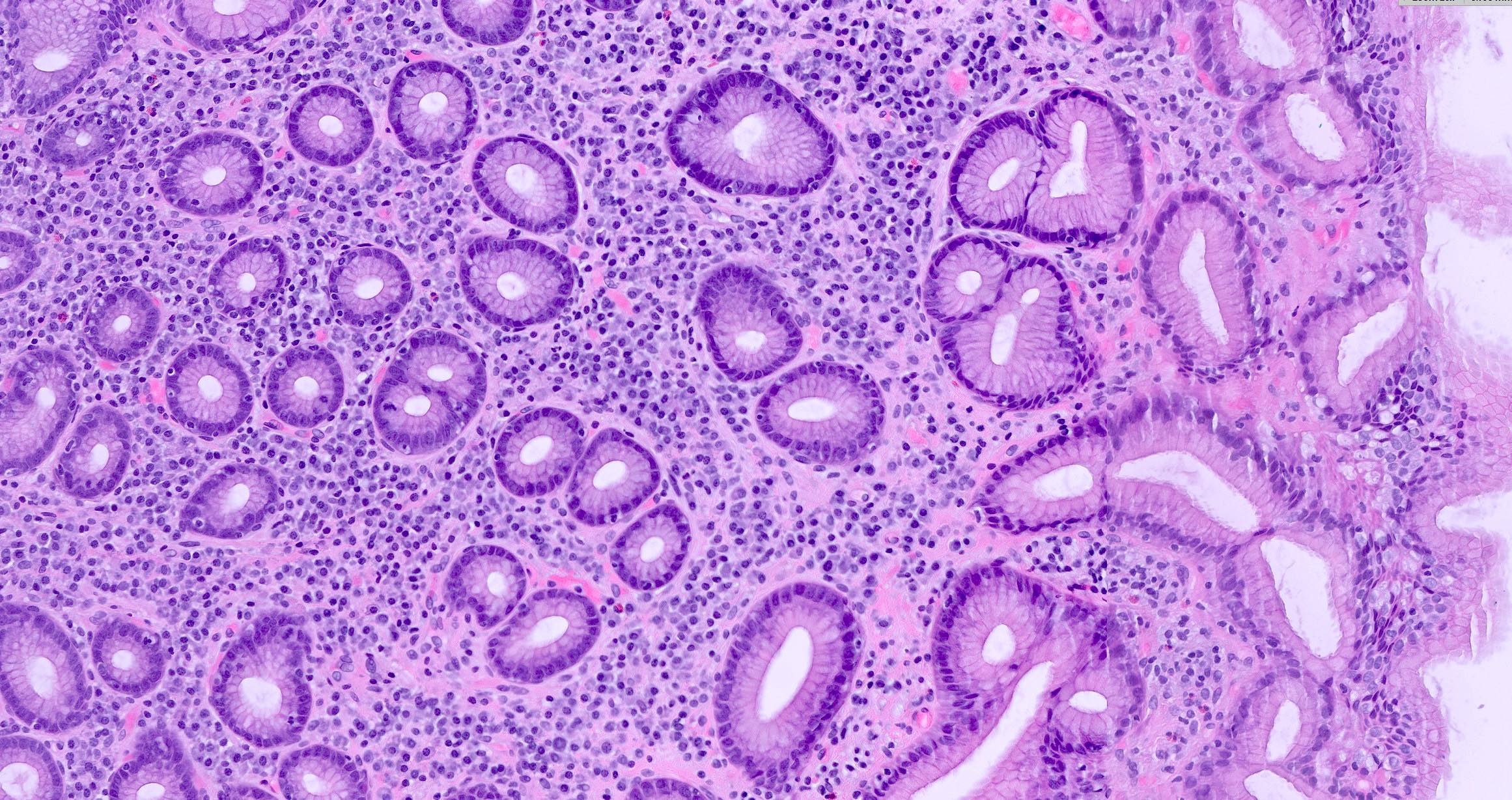
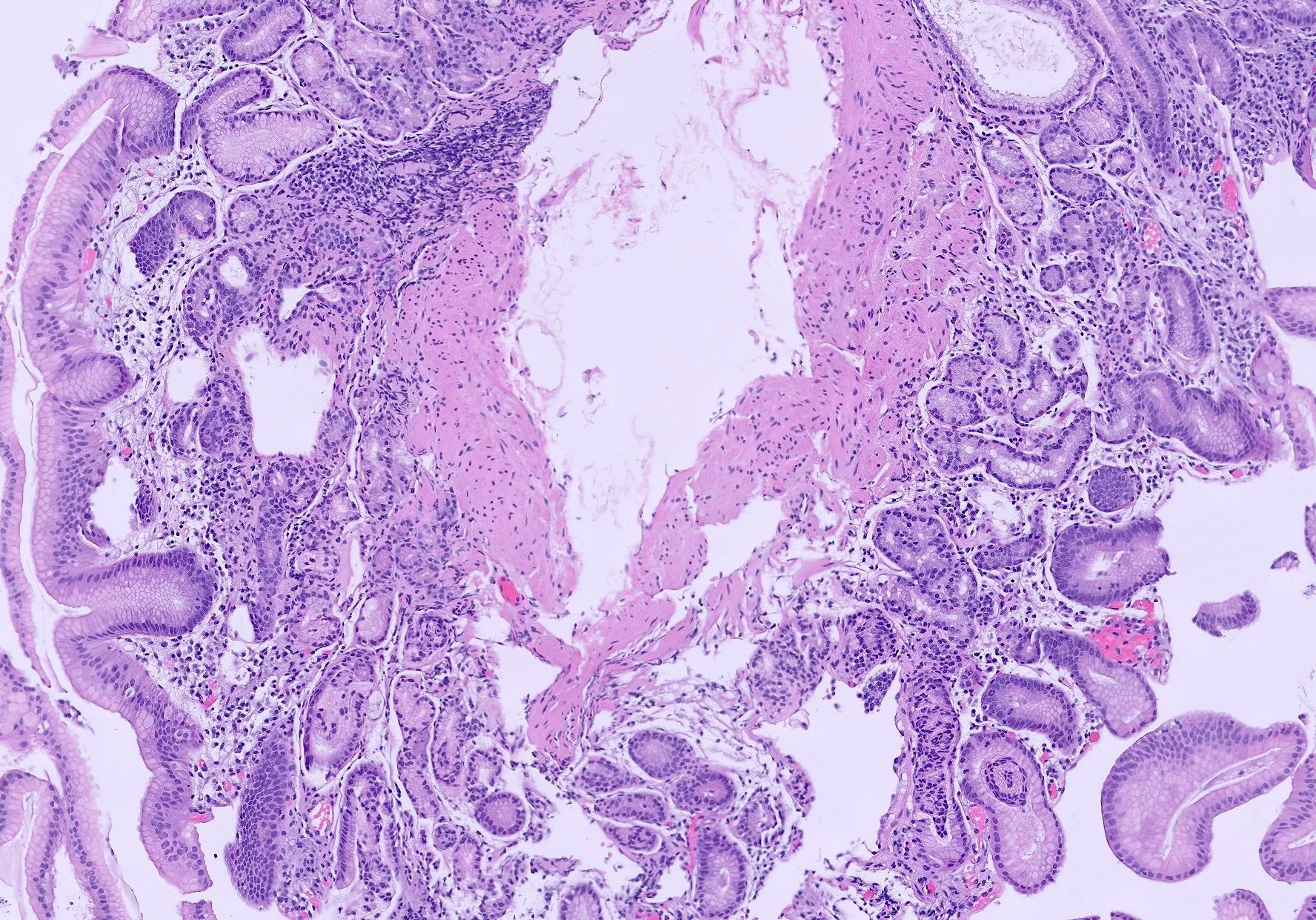
Image reference: PathologyOutlines.com
View topicDetailed Pathology
Definition
Gastritis is inflammation of the gastric mucosa, which can be acute (erosive) or chronic (predominantly lymphocytic). Chronic gastritis is most often caused by Helicobacter pylori infection or autoimmune mechanisms and can lead to atrophy, metaplasia, and increased cancer risk.
General / Essential Features
- Acute gastritis: neutrophil infiltration, mucosal erosions, haemorrhage
- Chronic gastritis: lymphoplasmacytic infiltrate, lymphoid follicles, glandular atrophy
- H. pylori gastritis: organisms visible on Giemsa stain, activity (neutrophils) in pit epithelium
- Autoimmune gastritis: body predominant, parietal cell loss, enterochromaffin-like (ECL) cell hyperplasia
- Intestinal metaplasia: goblet cells, Paneth cells – precursor to adenocarcinoma
- Reactive gastropathy: foveolar hyperplasia, minimal inflammation – due to bile reflux or NSAIDs
Sites
- Antrum (H. pylori gastritis)
- Body/fundus (autoimmune gastritis)
- Pylorus (reactive gastropathy)
Pathophysiology
H. pylori urease produces ammonia, damaging epithelium and recruiting neutrophils. Cytotoxin-associated gene A (CagA) strains increase cancer risk. Autoimmune gastritis results from autoantibodies against parietal cell H+/K+ ATPase and intrinsic factor, leading to vitamin B12 deficiency and pernicious anaemia.
Etiology
- H. pylori infection (most common)
- Autoimmune (parietal cell antibodies)
- NSAIDs, alcohol, bile reflux (reactive gastropathy)
- Stress (acute erosive gastritis)
- Crohn's disease (rarely)
Clinical Features
- Often asymptomatic
- Epigastric pain, nausea, bloating
- Haematemesis or melena in erosive gastritis
- Autoimmune: symptoms of pernicious anaemia (fatigue, neuropathy)
- Iron deficiency anaemia from chronic blood loss
Diagnosis
- Upper GI endoscopy with biopsy (gold standard)
- Rapid urease test / CLO test for H. pylori
- Histology: H&E, Giemsa or immunohistochemistry for H. pylori
- Serology: anti-parietal cell antibodies, anti-intrinsic factor antibodies
- Urea breath test or stool antigen for H. pylori
Treatment
- H. pylori eradication: triple therapy (PPI + amoxicillin + clarithromycin) for 14 days
- PPIs for symptom control
- Avoid NSAIDs, alcohol
- Iron or vitamin B12 supplementation if deficient
- Endoscopic surveillance for atrophic gastritis with metaplasia
Video Lesson
References
- Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. 2020.
- Harsh Mohan. Textbook of Pathology (8th ed.). Jaypee Brothers. 2019.
- Bancroft JD, Layton C. Bancroft's Theory and Practice of Histological Techniques (8th ed.). Elsevier. 2019.
- PathologyOutlines.com. (2024). View topic
Ready to test yourself?
Apply what you've learned in the Pathology Spotting Test