Red Blood Cells (RBCs)
Lesson 9 of 16 · Detailed theory + identification points
Points of Identification
4 pointsDetailed Theory
Object: Examination of Histological Slide of Red Blood Cells (RBCs)
General Overview
Red blood cells (erythrocytes) are the most numerous formed elements of blood (~5 million/µL in males, ~4.5 million/µL in females). Their primary function is transport of O₂ from the lungs to tissues and CO₂ from tissues back to the lungs, achieved via haemoglobin (Hb). They are the simplest cells in the body — highly specialised and enucleated at maturity.
Structure of the Mature RBC
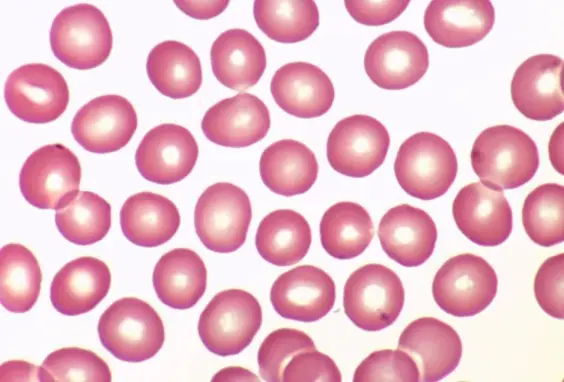
1. Shape — Biconcave Disc
Mature RBCs are anucleate biconcave discs approximately 7–8 µm in diameter and 2 µm thick at the rim, 1 µm at the centre. The biconcave shape: (a) maximises surface-area-to-volume ratio (~140 µm² surface area) for rapid gas diffusion; (b) creates a central pale zone (area of central pallor) on H&E stained smears due to the thinness at the centre; (c) allows deformation to pass through capillaries as narrow as 3 µm.
2. Haemoglobin and Eosinophilic Staining
Each RBC contains ~280 million Hb molecules. Hb is an eosinophilic protein (stains pink/red with eosin in H&E staining), giving RBCs their characteristic red colour on peripheral blood smears and histological sections. Each Hb molecule has 4 globin chains (2α + 2β in adult HbA) and 4 haem groups, each containing an Fe²⁺ ion that binds one O₂ molecule.
3. Cell Membrane and Flexibility
The RBC membrane is a lipid bilayer reinforced by a cytoskeletal meshwork of spectrin heterodimers, ankyrin, and protein 4.1 — giving it exceptional flexibility and durability. This allows RBCs to deform and recover their shape millions of times during their 120-day lifespan. Membrane proteins include glycophorin A (carries MN blood group antigens), Band 3 (anion exchanger for CO₂ transport as bicarbonate), and ABO blood group antigens.
4. Absence of Nucleus and Organelles
Mature RBCs have no nucleus, mitochondria, ribosomes, or endoplasmic reticulum. They cannot divide or synthesise proteins. They rely entirely on anaerobic glycolysis for ATP production (Embden-Meyerhof pathway) and on the pentose phosphate pathway to generate NADPH (protecting against oxidative damage via glutathione).
Erythropoiesis (Development)
RBCs develop from pluripotent haematopoietic stem cells in the bone marrow. Stages: proerythroblast → basophilic erythroblast → polychromatic erythroblast → orthochromatic erythroblast → reticulocyte (released into blood) → mature RBC. Nucleus is extruded at the orthochromatic erythroblast stage. Reticulocytes retain residual RNA (stained by new methylene blue) and mature within 1–2 days in the blood.
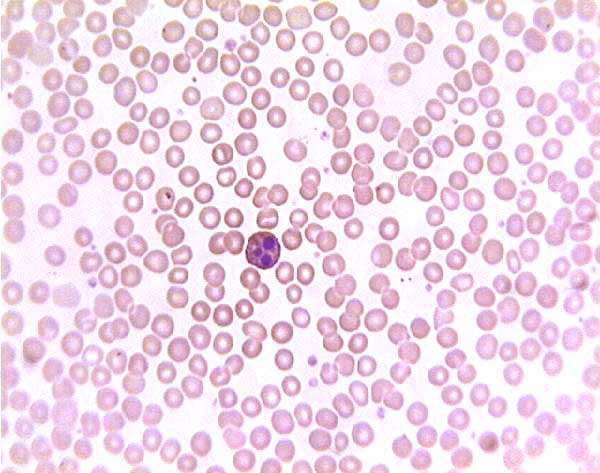
On a Stained Blood Smear (H&E / Giemsa)
- Eosinophilic (pink-red) cytoplasm throughout
- Central pallor — pale central zone occupying ~1/3 of the cell diameter (larger pallor = hypochromic anaemia)
- Uniform size — anisocytosis indicates pathology
- No nucleus — nucleated RBCs in adults = pathological
- 7–8 µm diameter — used as a scale reference for other cells (lymphocyte nucleus ≈ 1 RBC width)
Pathological Variations
- Microcytes: <6 µm — iron deficiency anaemia, thalassaemia.
- Macrocytes: >9 µm — B₁₂/folate deficiency.
- Sickle cells: Crescent shape — HbS (Val→Glu substitution at β6).
- Spherocytes: Loss of central pallor — hereditary spherocytosis, autoimmune haemolytic anaemia.
- Target cells: Central dense spot — liver disease, thalassaemia, HbC.
Video Lesson
Red Blood Cells (RBCs) — Histology Video Lesson
Click to play video lesson
References
4 sources- 1
Ross MH, Pawlina W. Histology: A Text and Atlas (8th ed.). Wolters Kluwer; 2020.
- 2
Young B, O'Dowd G, Woodford P. Wheater's Functional Histology (6th ed.). Churchill Livingstone/Elsevier; 2014.
- 3
Hoffbrand AV, Moss PAH. Essential Haematology (7th ed.). Wiley-Blackwell; 2016.
- 4
Junqueira LC, Carneiro J. Basic Histology: Text & Atlas (13th ed.). McGraw-Hill; 2013.
Disclaimer: These notes are for educational purposes only and compiled from standard histology textbooks. Clinical interpretation of slides requires a qualified histologist or pathologist.
Ready to test yourself?
Apply what you've learned in the Histology Spotting Test