Gall Bladder
Lesson 15 of 16 · Detailed theory + identification points
Points of Identification
6 pointsDetailed Theory
GALL BLADDER
General Overview
The gall bladder is a pear-shaped, hollow organ nestled in a fossa on the visceral surface of the liver. It functions to store, concentrate, and release bile into the duodenum in response to cholecystokinin (CCK) after a meal. It has a capacity of ~30–50 mL and can concentrate bile up to 10-fold by absorbing water and electrolytes. Embryologically, it derives from the hepatic diverticulum of the foregut.
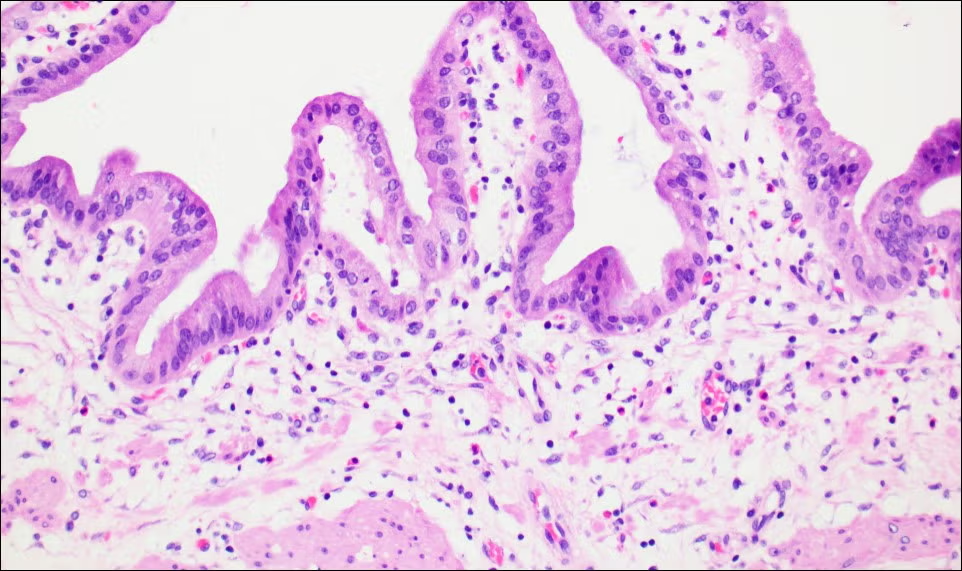
Histological Layers of the Gall Bladder Wall
The gall bladder wall is simpler than the rest of the gastrointestinal tract — it lacks a submucosa and a muscularis mucosae. The layers from lumen outward are summarised in the table below.
| Layer | Components | Key Features | Function / Notes |
|---|---|---|---|
| Mucosa | Simple tall columnar epithelium + lamina propria | No goblet cells; microvilli present; lamina propria with capillaries, lymphatics | Absorption of water/electrolytes; concentrates bile |
| Muscularis Propria | Smooth muscle bundles (oblique/longitudinal) | Thin, disorganised; no clear inner/outer layers | Contraction ejects bile into cystic duct (CCK-mediated) |
| Perimuscular Connective Tissue | Dense connective tissue with vessels, nerves | Replaces submucosa; continuous with liver adventitia | Provides support; contains parasympathetic ganglia |
| Serosa / Adventitia | Mesothelium (serosa) or fibrous (adventitia) | Serosa on free surface; adventitia where attached to liver | Reduces friction; anchors gall bladder |
Regional Variations
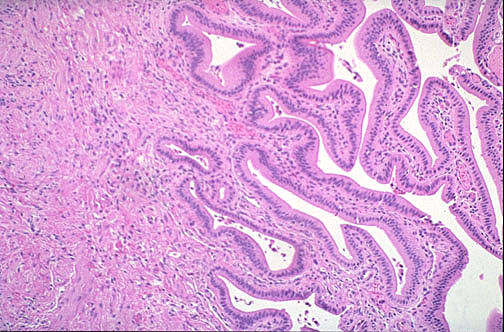
- Fundus/Body: Tall, elaborate mucosal folds; no glands in lamina propria.
- Neck (Infundibulum): Lower, less elaborate folds; contains mucous glands that secrete a thin mucus. Also present are small diverticula called Rokitansky–Aschoff sinuses — normal invaginations of epithelium through the muscularis propria that become more prominent and inflamed in chronic cholecystitis.
Ultrastructure and Function
- Apical microvilli: Amplify absorptive surface; contain enzymes (e.g., alkaline phosphatase).
- Tight junctions: Prevent back‑leakage of concentrated bile components.
- Lateral interdigitations and aquaporins: Facilitate rapid water and electrolyte transport (Na⁺-coupled absorption via Na⁺/H⁺ exchanger and Na⁺-K⁺-ATPase).
- Mitochondria: Abundant in the basal cytoplasm — energy for active transport.
Distinguishing Features from Small Intestine
- No villi or crypts — only tall mucosal folds (rugae).
- No goblet cells (intestine has many).
- No Paneth cells, no enteroendocrine cells (except occasional neuroendocrine cells).
- No submucosa or muscularis mucosae (intestine has both).
- Muscularis propria is thin and disorganised (intestine has distinct circular and longitudinal layers).
Clinical Correlations
- Cholelithiasis (gallstones): Most common disorder; cholesterol stones form when bile becomes supersaturated. Histologically, the mucosa may show signs of chronic inflammation.
- Chronic cholecystitis: Thickened wall with fibrosis, chronic inflammatory infiltrate, and prominent Rokitansky–Aschoff sinuses (epithelial invaginations deep into or through the muscularis propria).
- Cholesterolosis ("strawberry gallbladder"): Accumulation of lipid-laden macrophages in the lamina propria, giving a yellow‑speckled appearance on gross examination.
- Gallbladder adenocarcinoma: Rare, but arises most often in the neck; histologically shows gland‑forming malignant epithelium invading through the wall.
Summary Checklist for Slide Identification
- ✓ Tall, branching mucosal folds (not villi)
- ✓ Simple columnar epithelium — NO goblet cells
- ✓ Lamina propria with no glands (in body/fundus)
- ✓ Thin, poorly organised smooth muscle layer
- ✓ No submucosa — muscularis directly contacts perimuscular tissue
- ✓ In pathological specimens: Rokitansky–Aschoff sinuses (epithelial herniations)
References
5 sources- 1
Ross MH, Pawlina W. Histology: A Text and Atlas (8th ed.). Wolters Kluwer; 2020.
- 2
Young B, O'Dowd G, Woodford P. Wheater's Functional Histology (6th ed.). Churchill Livingstone/Elsevier; 2014.
- 3
Junqueira LC, Carneiro J. Basic Histology: Text & Atlas (13th ed.). McGraw-Hill; 2013.
- 4
Eroschenko VP. diFiore's Atlas of Histology with Functional Correlations (13th ed.). Wolters Kluwer; 2017.
- 5
Stricker TP, Kumar V. Robbins Basic Pathology (10th ed.). Elsevier; 2017.
Disclaimer: These notes are for educational purposes only and compiled from standard histology textbooks. Clinical interpretation of slides requires a qualified histologist or pathologist.
Ready to test yourself?
Apply what you've learned in the Histology Spotting Test